-
Adopt
-
Veterinary Care
Services
Client Information
- What to Expect – Angell Boston
- Client Rights and Responsibilities
- Payments / Financial Assistance
- Pharmacy
- Client Policies
- Our Doctors
- Grief Support / Counseling
- Directions and Parking
- Helpful “How-to” Pet Care
Online Payments
Referrals
- Referral Forms/Contact
- Direct Connect
- Referring Veterinarian Portal
- Clinical Articles
- Partners in Care Newsletter
CE, Internships & Alumni Info
CE Seminar Schedule
Emergency: Boston
Emergency: Waltham
Poison Control Hotline
-
Programs & Resources
- Careers
-
Donate Now
 Sue Casale, DVM, DACVS
Sue Casale, DVM, DACVS
Angell Animal Medical Center
617-541-5048
surgery@angell.org
Ureteral obstruction is becoming increasingly more common in veterinary patients and can occur for a variety of reasons.1,2 Although obstruction may be extra-luminal (accidental ligation, compression from mass) or intramural (neoplasia, polyps, ureterocele), the most common type of ureteral obstruction is intraluminal due to calculi.3,4 Ureteral obstruction is seen more commonly in cats than dogs which may be due to the small size of the feline ureter as well as the high likelihood that their calculi are composed of calcium oxalate, which cannot be dissolved medically. A majority of the ureteroliths seen in veterinary patients are composed of calcium oxalate, and in cats the incidence has been reported as high as 98%.2
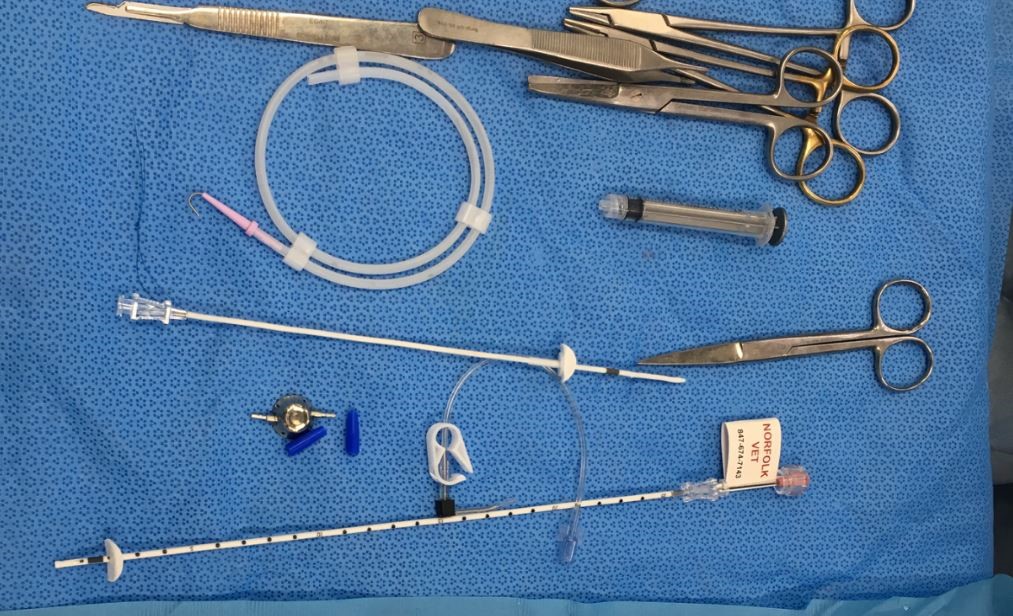
Subcutaneous Ureteral Bypass (SUB) device
Dogs with ureteral obstruction often present with urinary signs such as hematuria, pollakiuria, polyuria, and stranguria while cats tend to have more non-specific signs.4 Lethargy, anorexia, weight loss, vomiting may accompany urinary signs or may be the only presenting signs.4 This can make diagnosis difficult and will often delay surgical intervention. Azotemia is a common finding and is present in 83% of cats and 50% of dogs with unilateral obstruction.2 Anemia (cats), hyperphosphatemia, and hyperkalemia are also typical. Infection is more common in dogs than cats. Radiographs may show ureteral and renal calculi however abdominal ultrasound is the primary method used for diagnosis and should be performed on all patients with a suspected ureteral obstruction.5 Advanced imaging such as CT excretory urography is standard for humans but in veterinary patients ultrasound has similar sensitivity for ureteral dilation as CT and is more widely available.4
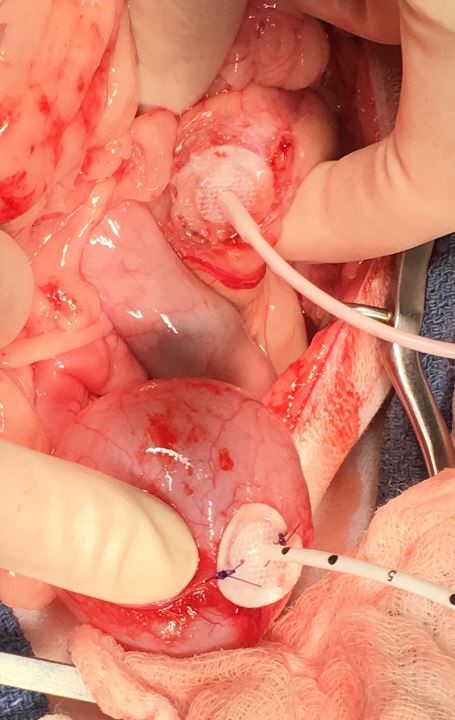
The nephrostomy (top) and cystotomy (bottom) catheters during surgery
Ureteral obstruction may be partial or complete. Complete ureteral obstruction requires emergent treatment because of the risk of permanent damage to the kidney. Following complete unilateral ureteral obstruction, renal blood flow gradually declines and by two weeks post obstruction, renal blood flow is only 20% of normal.6 Glomerular filtration rate (GFR) decreases in the affected kidney and increases in the contralateral kidney. GFR can return to normal if the obstruction is relieved within 4 days.6 Once an obstruction has been present for two weeks, permanent damage occurs and although GFR will improve after the obstruction has been relieved, it remains less than 50% of normal in previously healthy animals.6 In animals with pre-existing renal disease, this damage may be even more severe. Partial obstruction also requires immediate medical attention even though hydroureter or hydronephrosis may not be present.3 Renal damage and decreased GFR still occurs although the damage is slower and less severe. Recovery from partial obstruction is more complete even with delayed intervention. Experimentally, after 4 weeks of partial obstruction, GFR returned to normal once the obstruction was relieved.6

SUB port and Huber (non-coring) needle
Ureteral stenting with a double pig-tail stent has been reported and can be considered.10 Stents are placed either retrograde using cystoscopic guidance, antegrade through the renal pelvis, or surgically.3 Success appears to be very good in dogs but the procedure is technically challenging in cats due to the small size of the feline ureter.11,12,13 The perioperative complication rate with stents is lower than ureteral surgery (10-14%) but long-term complications, are high with dysuria (17-35%), urinary tract infections (20%), recurrent obstruction (22%) and stent migration (5%) being the most common.3,14,15
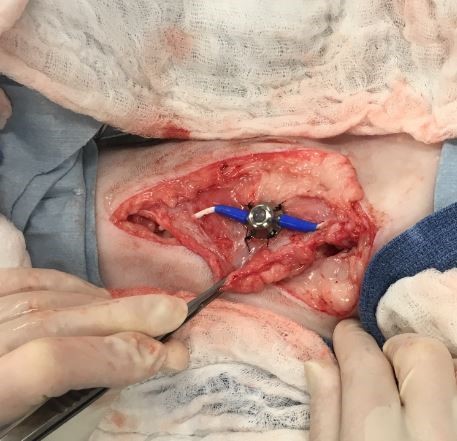
The SUB port sutured subcutaneously to the body wall
The newest technique to treat ureteral obstruction is the subcutaneous ureteral bypass (SUB™) system.3,12 Developed over 10 years ago based on a subcutaneous nephrovesical bypass used in human urology, the SUB device has shown improved outcome and decreased complications in cats when compared to ureteral stents.13,16,17,18 The SUB™ device consists of placement of a locking loop nephrostomy catheter within the renal pelvis and a cystotomy catheter within the bladder. The two catheters are connected by a port that is placed subcutaneously.18 The port is easily palpated under the skin and is accessed with a Huber needle to prevent coring. Urine can be easily sampled and the system can be checked/flushed to minimize the risk of the catheters becoming occluded. The nephrostomy catheter is a 6 French pigtail catheter that is placed into the renal pelvis with or without fluoroscopic guidance.18,19 A dacron cuff is glued to the renal capsule to prevent leakage and to secure the catheter in place. The bladder catheter also has a dacron cuff that is both glued and sutured to the urinary bladder.18 The SUB is available in both a single port for unilateral obstruction and a 3-way PantsPort™ for bilateral obstruction. The PantsPort™ allows a nephrostomy tube from each kidney to drain into a single cystotomy catheter.18

Post-operative radiograph showing SUB placement
Complications are rare but include leakage (<5%) in the immediate post-operative period from the nephrostomy catheter, cystotomy catheter or the port attachment, kinking of the device (<3%) and obstruction of the SUB (15-20%) with debris/stones/blood clots.13,20 The rate of post-operative obstruction is decreased with regular flushing of the device.18 Dysuria, which is the most common long term complications seen with the double pigtail stent, is rare after SUB placement (<5%).13 Regular postoperative maintenance of the SUB is necessary. The device should be flushed under ultrasound or fluoroscopic guidance to avoid over-distention of the renal pelvis, every 3 to 6 months to confirm patency of the device.18 A urine sample, which is easily obtained at the time of flushing, should be submitted for culture.18

Post-operative radiograph showing SUB placement
Excellent results were reported for a series of 137 cats that had SUB placement for ureteral obstruction.21 Over 93% of the cats survived to discharge.21 Renal pelvis dilation resolved and improvement in azotemia was seen. In one study, creatinine levels dropped 77.3% between admission and discharge from the hospital.19 Cats with more severe renal disease have worse long term survival.20 Owner satisfaction following the SUB procedure is high (>90%).19 We have been implanting SUB devices at Angell Animal Medical Center for over two years with good success. It has quickly become our preferred treatment for cats with ureteral obstruction. The SUB device can also be used in dogs for treatment of ureteral obstruction that cannot be treated with stents or traditional surgery.
For more information about Angell’s Surgery service, please visit angell.org/surgery. Dr. Casale can be reached at 617-541-5048, or by e-mailing scasale@angell.org or surgery@angell.org.
References:
- Cannon AB, Westropp JL, Ruby AL, and Kass PH. Evaluation of trends in urolith composition in cats: 5,230 cases (1985-2004). J Am Vet Med Assoc 2007; 231(4): 570-576.
- Kyles, AE, Hardie, EM, Wooden, BG, Adin CA, et al. Clinical, clinocopathologic, radiographic, and ultrasonographic abnormalities in cats with ureteral calculi: 163 cases (1984-2002). J Am Vet Med Assoc 2005; 226(6): 932-936.
- Berent, AC. Ureteral obstructions in dogs and cats: a review of traditional and new interventional diagnostic and therapeutic options. J of Vet Emerg Critical Care 2011; 21(2): 86-103.
- Hardie, EM and Kyles, AE. Management of ureteral obstruction. Vet Clin North Am Small Anim Pract 2004; 34: 989-1010.
- Palm, CA, Culp, WTN. Nephroureteral obstructions. The use of stents and ureteral bupass systems for renal decompression. Vet Clin North Am Small Anim Pract 2016; 46: 1183-1192.
- Wen JG, Frokiaer, J, Jorgensen, TM, et al. Obstructive nephropathy: an update of the experimental research. Urol Res 1999; 27: 29-39.
- Kyles, AE, Hardie, EM, Woden, BG, Adin, CA, et al. Management and outcome of cats with ureteral calculi: 153 cases (1984-2002). J Am Vet Med Assoc 2005; 226(6): 937-944.
- Roberts, SF, Aronson, LR and Brown, DC. Postoperative mortality in cats after uerterolithotomy. Vet Surg 2011; 40: 438-443.
- Garcia de Carellan Mateo, A., Brodbelt, D., Kulendra, N. and Alibhai, H. Retrospective study of the perioperative management and complications of ureteral obstruction in 37 cats. Vet Anaesth Analg 2015; 42: 570–579.
- Manassero, M, Decambron, A, Viateau, V, Bedu, AS et al. Indwelling double pigtail ureteral stent combined or not with surgery for feline ureterolithiasis: complications and outcome in 15 cases. J Fel Med Surg 2014; 16(8): 623-630.
- Kuntz, JA, Berent, AC, Weisse, CW, Bagley, DH. Double pigtail ureteral stenting and renal pelvic lavage for renal-sparing treatment of obstructive pyomephritis in dogs: 13 cases (2008-2012). J Am Vet Med Assoc 2025; 246(2): 216-225.
- Berent, AC. Interventional radiology and interventional endoscopy of the urinary tract (‘endourology’). J Fel Med Surg 2014; 16: 51-65.
- Berent, AC Treatment of feline ureteral obstructions: stents versus SUBs – the last 10 years of experience. Proceedings of ACVIM, Denver CO, 2016
- Kulendra, NJ, Syme, H, Benigni, L, Halfacree, Z. Feline double pigtail ureteric stents for management of ureteric obstruction: short-and long-term follow-up of 26 cats. J Fel Med Surg 2014; 16: 985-991.
- Wormser, C, Clarke, DL, Aronson, LR. Outcomes of ureteral surgery and ureteral stenting in cats: 117 cases (2006-2014). J Am Vet Med Assoc 2016; 248(5): 518-525.
- Schmidbauer, J Kratzik, C, Klinger, HC, et al. Nephrovesicical subcutaneous ureteric bypass: long-term results in patients with advanced metastatic disease – improvement of renal function and quality of life. Eur Urol 2006; 50:1073-1078.
- Komiakov, BK, Guliev, BG, El’-Attar, TKh, et al. Subcutaneous nephrovesical bypass in ureteral obstruction. Urologiia 2009; 5: 3-8.
- Berent, A, Weisse, C. Subcutaneous ureteral bypass system – a surgical guide. Norfolk Vet Products, Skokie, IL.
- Livet, V, Pillard, P, Goy-Thollot, I, Maleca, D, et al. Placement of subcutaneous ureteral bypasses without fluoroscopic guidance in cats with ureteral obstruction: 19 cases (2014-2016). J Fel Med Surg 2016; 18: 1-10.
- Horowitz, C, Berent, A, Weisse, C, Langston, C, Bagley, D. Predictors of outcome for cats with ureteral obstructions after interventional management using ureteral stents or a subcutaneous ureteral bypass device. J Fel Med Surg 2015; 15(12): 1052-1062.
- Berent, AC, Weisse, C, Bagley, D. Subcutaneous ureteral bypass device placement for benign ureteral obstruction in cats: 137 cats (174 ureters). Proceedings of ACVIM, Denver CO, 2016