-
Adopt
-
Veterinary Care
Services
Client Information
- What to Expect – Angell Boston
- Client Rights and Responsibilities
- Payments / Financial Assistance
- Pharmacy
- Client Policies
- Our Doctors
- Grief Support / Counseling
- Directions and Parking
- Helpful “How-to” Pet Care
Online Payments
Emergency: Boston
Emergency: Waltham
Poison Control Hotline
-
Programs & Resources
- Careers
-
Donate Now
 By Callie Cazlan Verschoor, DVM
By Callie Cazlan Verschoor, DVM![]()
angell.org/urgentcare
urgentcare@angell.org
617-522-7282
March 2024
x
x
Emergency clinic veterinarians know the feeling when a 12-year-old Labrador retriever walks into the clinic with a presenting complaint such as “wobbly in back legs, not eating.” Said Labrador is then  triaged, and veterinarians find pale mucous membranes leading to a fast scan that identifies ascites that aspirates as blood. The non-traumatic hemoabdomen (spontaneous hemoperitoneum (SHP)) has been an area of extensive study as this is not an uncommon case to encounter during an emergency shift. It is also one that comes with high emotional weight, so it is important that we understand what is available to these patients. This article will concentrate on updates over the past five years regarding the management of non-traumatic hemoabdomen and prognostic indicators.
triaged, and veterinarians find pale mucous membranes leading to a fast scan that identifies ascites that aspirates as blood. The non-traumatic hemoabdomen (spontaneous hemoperitoneum (SHP)) has been an area of extensive study as this is not an uncommon case to encounter during an emergency shift. It is also one that comes with high emotional weight, so it is important that we understand what is available to these patients. This article will concentrate on updates over the past five years regarding the management of non-traumatic hemoabdomen and prognostic indicators.
If a client expresses interest in going to surgery, a veterinarian will likely start to ponder the value of pre-operative imaging of the abdomen. Most commonly, if available, clinicians will reach for an abdominal ultrasound (AUS) to identify the source of bleeding and evaluate for gross metastasis. But how helpful is this?
In February 2021, a study5 evaluated the diagnostic utility of ultrasound to answer this question. Medical records from 94 client-owned dogs were evaluated for differences between AUS, surgical, and necropsy findings. The study identified that splenic masses were most commonly identified as the cause of the SHP. The sensitivity of AUS was 87.4%, 37.3%, and 31.3% for masses in the spleen, liver, and mesentery, respectively. Notably, zero of six dogs with peritoneal diffuse nodular metastasis had lesions detected by AUS. As such, it can be concluded that AUS is not very sensitive for nodular metastasis but is for splenic masses (which is the most common). For most clients, an ultrasound report with nodular metastasis would halt the plan for surgical treatment. With that said, only six of the 94 dogs had nodular metastasis, so it might be considered somewhat rare in SHP cases. However, the risk must be weighed, as clinicians will not fully be able to answer the question of metastasis on a pre-operative ultrasound, and the client should be warned of such risk. Additionally, it can be considered to forego the pre-operative abdominal ultrasound if it is not available (or a client has limited finances) as it is not a 100% sensitive modality for assessing metastasis. Gross evaluation during surgery is the only way to evaluate fully.
As clinicians gather point-of-care information on the patient, they will likely run a PCV/TP as part of their database. The decision of when or if to consider a packed red blood transfusion (pRBC) can be one of debate. A study2 published in 2022 reviewed admission total plasma protein as a predictor of red blood cell transfusion requirements in both traumatic and non-traumatic hemoabdomens. Ninety dogs were retrospectively evaluated. A total of 47 dogs (traumatic hemoabdomen 11/26; non-traumatic 36/64) received pRBC transfusions. For each 1 g/dL unit decrease in TP, dogs had an increased odds ratio of 2.14 of receiving a transfusion. Lower PCV, bicarbonate values, base excess, and higher lactate were also associated with increased transfusion rate. As such, it was concluded that lower admission TP values,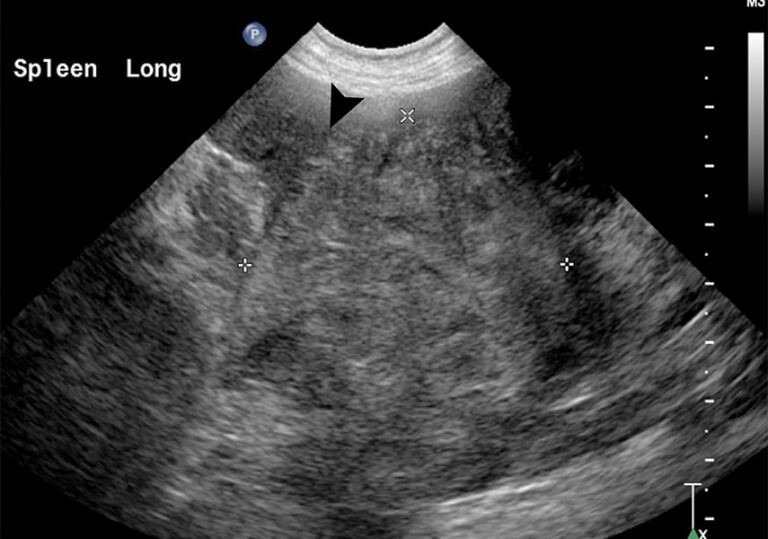 independent of low PCV, were associated with increased red blood cell transfusion. Clinically, you might consider preparing for red blood cell transfusion or even pro-actively administering a pRBC transfusion if the total protein is low despite the PCV. In this paper, a TP of <5.6 g/dL was associated with an increased rate of pRBC administration vs a TP of >6.1 in those that did not. This ultimately may lead to better post-operative and surgical outcomes if we stay ahead of blood loss. PCV/TP is also a technically accessible and cost-effective test for running point of care and is part of a workup for any SHP case.
independent of low PCV, were associated with increased red blood cell transfusion. Clinically, you might consider preparing for red blood cell transfusion or even pro-actively administering a pRBC transfusion if the total protein is low despite the PCV. In this paper, a TP of <5.6 g/dL was associated with an increased rate of pRBC administration vs a TP of >6.1 in those that did not. This ultimately may lead to better post-operative and surgical outcomes if we stay ahead of blood loss. PCV/TP is also a technically accessible and cost-effective test for running point of care and is part of a workup for any SHP case.
The last update to touch on is tranexamic acid (TXA), a synthetic derivative of the amino acid lysine that inhibits fibrinolysis. This is still an area of debate and study, but this author will highlight a few papers on this topic published recently. Hyperfibrinolysis (HF) is when the body dissolves hemostatic fibrin, resulting in excessive or recurrent bleeding. It has been established that, likely in the initial diagnosis of SHP, dogs have a hyperfibrinolytic state, but the prevalence and duration were unknown. A study1 published in 2022 showed that HF occurs in some dogs with hypovolemic shock due to SHP but resolves rapidly following surgical control of bleeding. This was determined by measuring PCV, total plasma protein, platelet count, and thromboelastography with 50 U/mL plasminogen activator at presentation and then every eight hours post-operatively until 72 hours, discharge or death. This proves that post-operatively, TXA is not likely to be of benefit to patients since HF resolves with surgical treatment. But what about pre-operatively? Another study in 20203 reviewed the use of TXA in critically ill dogs and cats. Administration of TXA before or after pRBC transfusion did not significantly affect the median dose of pRBC administration. Adverse reactions were mild and rare in this study; the average dose was 10 mg/kg. While these conclusions help determine that TXA is a well-tolerated drug, clinicians do not know if it truly contributes to better clinical outcomes. This paper shows that the need for transfusion was not significantly lower. In human medicine, in 2013, the CRASH 2 study4 has been cited, which showed that early administration for adults with traumatic bleeding reduced the risk of death. This may be extrapolated to cases of traumatic hemoabdomen, but in veterinary medicine, doctors do not have a clinical trial for comparison. All this is to say that clinically, TXA is well tolerated and may have a benefit, but none has been proven. It likely does not have a benefit for post-operative use but may be considered pre-operatively as clinicians have not fully evaluated its benefit pre-op.
Cases of SHP can be some of the most rewarding with good stabilization techniques and surgical correction. Consider ultrasound’s sensitivity in pre-operative metastasis evaluation for a future case and factor this into the conversation with clients. Another suggestion is to double-take at a low TPP and prepare for a pRBC transfusion. Also, maybe consider the use of pre-operative TXA if the patient is showing evidence of shock. But likely not post-operatively, as it has been proven the hyperfibrinolytic state resolves with surgical removal of the bleeding mass. It will be exciting to see ongoing research areas on this topic over the next five years as clinicians continue to learn how to approach it best.
References
1. Ian M. Destefano, E. A. (2022). Rapid resolution of hyperfibrinolysis in dogs with spontaneous hemoperitoneum following surgical correction of hemorrhage. Veterinary Emergency and Critical Care, 305-314.
2. Miranda Buseman, A. E. (2022). Retrospective evaluation of admission total plasma protein as a predictor of red blood cell transfusion requirement in dogs diagnosed with traumatic and nontraumatic hemoabdomen:90 dogs (2009-2019). Veterinary Emergency and Critical Care, 76-80.
3. Morgan Kelley DVM, V. S.-S. (2022). Retrospective analysis of the use of tranexamic acid in critically ill dogs and cats (2018-2019):266 dogs and 28 cats. Veterinary Emergency and Critical Care, 791-799.
4. Roberts I, Shakur H, Coats T, Hunt B, Balogun E, Barnetson L, Cook L, Kawahara T, Perel P, Prieto-Merino D, Ramos M, Cairns J, Guerriero C. The CRASH-2 trial: a randomised controlled trial and economic evaluation of the effects of tranexamic acid on death, vascular occlusive events and transfusion requirement in bleeding trauma patients. Health Technol Assess. 2013 Mar;17(10):1-79. doi: 10.3310/hta17100. PMID: 23477634; PMCID: PMC4780956.
5. Sarah E. Cudney, A. S. (2021). Diagnostic utility of abdominal ultrasonography for evaluation of dogs with nontraumatic hemoabdomen 94 cases (2014-2017). Journal of the American Veterinary Medical Association, 290-294.