-
Adopt
-
Veterinary Care
Services
Client Information
- What to Expect – Angell Boston
- Client Rights and Responsibilities
- Payments / Financial Assistance
- Pharmacy
- Client Policies
- Our Doctors
- Grief Support / Counseling
- Directions and Parking
- Helpful “How-to” Pet Care
Online Payments
Emergency: Boston
Emergency: Waltham
Poison Control Hotline
-
Programs & Resources
- Careers
-
Donate Now
 By Evan Mariotti, DVM, DACVIM (SAIM)
By Evan Mariotti, DVM, DACVIM (SAIM)![]()
angell.org/internalmedicine
internalmedicine@angell.org
617-541-5186
March 2021
In this article for primary care veterinarians, Dr. Evan Mariotti provides a summarized review of five congenital and pediatric endocrine diseases that affect dogs and cats.
Pituitary Dwarfism
 The German Shepherd Dog is the poster child for this disease. Genetically, this is due to an autosomal recessive mutation in the LHX3 gene. These dogs typically have combined GH, TSH, and prolactin deficiencies with impaired release of GNRH and LH. ACTH levels are normal. There may be evidence of cyst formation during the development of Rathke’s Pouch which can be seen on CT or MRI in addition to pituitary hypoplasia. Clinically, these dogs have a lack of primary guard hairs with retention of the puppy coat which leads to easy epilation and secondary bacterial infections. The males are cryptorchid from lack of GNRH release and the females are unable to ovulate due to lack of LH release. They also have AA malformation which may cause spinal cord compression. Secondary hypothyroidism leads to lack of activity at about 2-3 years of age but they are active and alert prior to this. The diagnosis comes from excluding other endocrine and non-endocrine causes for dwarfism and alopecia. These dogs have abnormal glomerular development with impaired renal function and an elevated creatinine. A DNA test for LHX3 is available which can be useful for diagnosis as well as screening for breeding animals. Definitive diagnosis of GH deficiency is a growth hormone stimulation test using GHRH or alpha-adrenergic drugs where GH levels are measured before and 20-30 minutes after administration. The treatment is porcine GH 0.1-0.3 IU/kg three times a week or Progestins but can lead to DM, mammary tumors, pyoderma, and skeletal developmental issues. There is improvement of skin and hair in 6-8 weeks. Growth depends on the status of the growth plates. Monitoring of GH, IGF-1 and glucose is important during therapy. The prognosis is poor leading to quality of life concerns by age 3-5 due to renal failure, pituitary cyst growth and poor haircoat. Treatment with L-thyroxine and porcine GH or progestins improved length of life but the prognosis still remains guarded.
The German Shepherd Dog is the poster child for this disease. Genetically, this is due to an autosomal recessive mutation in the LHX3 gene. These dogs typically have combined GH, TSH, and prolactin deficiencies with impaired release of GNRH and LH. ACTH levels are normal. There may be evidence of cyst formation during the development of Rathke’s Pouch which can be seen on CT or MRI in addition to pituitary hypoplasia. Clinically, these dogs have a lack of primary guard hairs with retention of the puppy coat which leads to easy epilation and secondary bacterial infections. The males are cryptorchid from lack of GNRH release and the females are unable to ovulate due to lack of LH release. They also have AA malformation which may cause spinal cord compression. Secondary hypothyroidism leads to lack of activity at about 2-3 years of age but they are active and alert prior to this. The diagnosis comes from excluding other endocrine and non-endocrine causes for dwarfism and alopecia. These dogs have abnormal glomerular development with impaired renal function and an elevated creatinine. A DNA test for LHX3 is available which can be useful for diagnosis as well as screening for breeding animals. Definitive diagnosis of GH deficiency is a growth hormone stimulation test using GHRH or alpha-adrenergic drugs where GH levels are measured before and 20-30 minutes after administration. The treatment is porcine GH 0.1-0.3 IU/kg three times a week or Progestins but can lead to DM, mammary tumors, pyoderma, and skeletal developmental issues. There is improvement of skin and hair in 6-8 weeks. Growth depends on the status of the growth plates. Monitoring of GH, IGF-1 and glucose is important during therapy. The prognosis is poor leading to quality of life concerns by age 3-5 due to renal failure, pituitary cyst growth and poor haircoat. Treatment with L-thyroxine and porcine GH or progestins improved length of life but the prognosis still remains guarded.
Diabetes Insipidus
 Arginine vasopressin is secreted from the posterior lobe of the pituitary gland. The main stimulus for release is an increase in plasma osmolality and can be suppressed by baroreceptors. DI is associated with decreased production or lack of action of AVP. Central diabetes insipidus is a complete or partial deficiency in AVP. Congenital central diabetes insipidus has been described in Afghan Hound littermates. Nephrogenic diabetes insipidus is characterized by decreased action of AVP. Familial NDI leads to alteration in aquaporin expression and possible involvement of decreased binding of AVP to V2. Congenital DI can be diagnosed at any age. These animals are profoundly PU/PD leading to nocturia and overflow incontinence. This in turn leads to medullary washout, lower than normal BUN and hyposthenuria. Diagnosis can be made using strict guidelines of a modified water deprivation test. The owners need to be aware of the risks of hypertonic dehydration before beginning the test. A DDAVP trial is a simple alternative where owners note water consumption before and during treatment and the USG should increase indicating a positive response. A positive result leads to animals being on DDAVP long-term with dose adjustments as needed. Treatment of NDI is with thiazide diuretics which decreases Na+ absorption and leads to increase water and sodium absorption in the proximal tubules.
Arginine vasopressin is secreted from the posterior lobe of the pituitary gland. The main stimulus for release is an increase in plasma osmolality and can be suppressed by baroreceptors. DI is associated with decreased production or lack of action of AVP. Central diabetes insipidus is a complete or partial deficiency in AVP. Congenital central diabetes insipidus has been described in Afghan Hound littermates. Nephrogenic diabetes insipidus is characterized by decreased action of AVP. Familial NDI leads to alteration in aquaporin expression and possible involvement of decreased binding of AVP to V2. Congenital DI can be diagnosed at any age. These animals are profoundly PU/PD leading to nocturia and overflow incontinence. This in turn leads to medullary washout, lower than normal BUN and hyposthenuria. Diagnosis can be made using strict guidelines of a modified water deprivation test. The owners need to be aware of the risks of hypertonic dehydration before beginning the test. A DDAVP trial is a simple alternative where owners note water consumption before and during treatment and the USG should increase indicating a positive response. A positive result leads to animals being on DDAVP long-term with dose adjustments as needed. Treatment of NDI is with thiazide diuretics which decreases Na+ absorption and leads to increase water and sodium absorption in the proximal tubules.
Hypoparathyroidism
Lack of parathyroid hormone leads to hypocalcemia and hyperphosphatemia. Dogs and cats with no known history of surgery or trauma have idiopathic hypoparathyroidism and some have an immune-mediated etiology. Dogs at the time of diagnosis have ranged from 6 weeks to 10-13yrs in age. Females, terriers, GSD, Poodles and miniature schnauzers are predisposed. Most clinical signs are related to neuromuscular signs such as tetany, seizures, and muscle fasciculation but also include panting, facial rubbing and behavioral. Diagnosis is by measuring tCa, iCa and PTH levels. These animals will have low iCa and tCa with inappropriately low PTH level. Dogs with severe hypocalcemia should have treatment initially with a calcium gluconate bolus followed with a CRI. Oral supplementation might also be required until calcitriol takes effect. They are then transitioned to calcium gluconate in maintenance IV fluids and then weaned onto oral calcium and calcitriol alone. Animals can usually be weaned off of the oral calcium supplementation and maintained on calcitriol alone.
Hypothyroidism
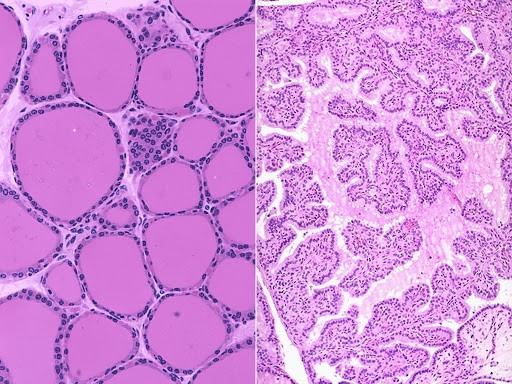
Normal vs. Hypothyroid
This a rare congenital disease that may be underrepresented in dogs. Often times, because thyroid hormone is essential for development, the dog dies at or shortly after birth. They have disproportionate dwarfism, mental impairments, constipation, and short uneven limbs. They are usually normal at birth but the disease becomes evident around 8 weeks of age. Goiter may or may not be present. Biochemical testing and results is the same as for acquired hypothyroidism. Dogs are usually debilitated from the disease and their prognosis remains poor but better with supplementation if diagnosed early in age. Cats also can have congenital dyshormonogenesis or dysmorphogenesis. They have similar clinical appearances as the dog and are often brought in for constipation and misdiagnosed with congenital megacolon. Diagnosis is with TT4, cTSH and if indicated, thyroid scintigraphy. Treatment
with L-thyroxine still leads to a guarded prognosis in cats.
Hypoadrenocorticism
Addison’s disease is characterized as a lack in glucocorticoid and mineralocorticoid production. Although this is primarily a disease of middle-aged dogs, we can also see this in the pediatric patient. There are a wide range of signs associated with HA including vomiting, diarrhea, PU/PD, and collapse. These animals can present with mild to severe signs of hypovolemia, dehydration and bradycardia. Useful diagnostic results include the lack of a stress leukogram, a lymphocytosis, isosthenuria and an Na:K ratio of less than 28. An ACTH stimulation test confirms the diagnosis. In the acute crisis, aggressive fluid therapy with 0.9% NaCl should be performed being careful not to raise sodium too quickly. Administer Dexamethasone as needed and DOCP once the patient is stable. Prednisone is administered orally once stable and tapered to a physiologic dose. Time between DOCP injections as well as dose can be lengthened and decreased respectively. Careful monitoring of these patients is required.