-
Adopt
-
Veterinary Care
Services
Client Information
- What to Expect – Angell Boston
- Client Rights and Responsibilities
- Payments / Financial Assistance
- Pharmacy
- Client Policies
- Our Doctors
- Grief Support / Counseling
- Directions and Parking
- Helpful “How-to” Pet Care
Online Payments
Emergency: Boston
Emergency: Waltham
Poison Control Hotline
-
Programs & Resources
- Careers
-
Donate Now
 By Sue Casale, DVM, DACVS-SA
By Sue Casale, DVM, DACVS-SA![]()
angell.org/surgery
surgery@angell.org
617-541-5048
May 2022
Swallowing is usually a well-coordinated sequence of movements involving the tongue, mouth muscles, palate, and pharynx.1,2 It consists of four phases: oral, pharyngeal, cricopharyngeal, and esophageal.2,3 Only the early oral phase is voluntary, and it consists of licking liquid or prehension, mastication, and lubrication of food.3 This is followed by contraction of the tongue, which elevates it to the hard palate, propelling the food bolus to the back of the mouth into the pharynx. During the pharyngeal phase, the soft palate is elevated to block off the nasopharynx from the oropharynx, the vocal folds close to seal the larynx, and the epiglottis covers the laryngeal opening.1,2 The pharyngeal muscles contract, moving the bolus toward the pharyngoesophageal junction and upper esophageal sphincter (UES), starting the cricopharyngeal phase.2 The UES is a striated muscle sphincter consisting of the cricopharyngeus muscle.4 This muscle is normally in a state of contraction, which prevents air entry into the esophagus and esophageal and gastric contents from entering the pharynx.4 Once the food bolus enters the pharynx, respiration stops briefly, and the UES relaxes, allowing the food to pass through the UES into the proximal esophagus.2 During the esophageal phase, the food bolus is moved abroad aided by peristalsis, which helps propel it into the stomach.
Dysphagia, or difficulty swallowing, can be caused by several different conditions. It is classified by its anatomic location and phase of swallowing. Dysphagia in the oral phase usually affects prehension and can be diagnosed by watching the patient eat or drink. For pharyngeal, cricopharyngeal, or esophageal dysphasia, advanced diagnostics are required to determine the source of the dysphagia. Cricopharyngeal achalasia is a rare type of dysphagia resulting from decreased compliance of the cricopharyngeal muscle.3 Incomplete relaxation of this muscle during swallowing results in difficulty moving food through the UES into the esophagus. The bolus of food remains in the pharynx, and repeated attempts at swallowing may allow some food to pass. However, there is also the risk of aspiration of ingesta into the airways.
Most dogs with cricopharyngeal achalasia have a ravenous appetite. However, after the prehension of food, the dogs experience multiple chewing and swallowing attempts followed by gagging, regurgitation, and coughing.2,3 They may also experience excessive salivation, an extension of their neck after food intake, and food falling from their mouths.3 One of the hallmark signs of cricopharyngeal achalasia is water coming out of the nose when drinking.2 This results from the pharynx muscles contracting against a closed UES resulting in reflux of liquid into the nasopharynx. Cricopharyngeal achalasia typically presents in young dogs, less than one year of age, and with signs typically noticed after weaning. The most commonly affected breeds are the Cocker and Springer Spaniel, Bouvier des Flandres, Golden Retriever, Dachshund, Maltese, and Miniature and Standard Poodles.2,3 Cricopharyngeal dysfunction has shown to be genetic in Cocker Spaniels and Golden Retrievers and caused by hereditary muscular dystrophy in Bouviers.5,6,7
Physical examination of dogs with cricopharyngeal achalasia is usually normal. Neurologic examination, oral examination, blood work, and survey thoracic and neck radiographs are recommended to help rule out other causes of dysphagia.2,3 Pharyngeal tumors, foreign bodies, laryngeal paralysis, cleft palate, and megaesophagus can be ruled out with a thorough sedated oral examination and radiographs.3 Hypothyroidism and myasthenia gravis have been linked with cricopharyngeal dysphagia and should be included in the differential diagnosis list, especially in older dogs.3,8 A thyroid panel, acetylcholinesterase receptor antibodies, and type 2 muscle autoantibodies should be submitted.3 Videofluoroscopic swallowing studies are necessary to differentiate cricopharyngeal dysphagia from pharyngeal dysphagia and rule out esophageal strictures and foreign bodies.9,10,11 This test is performed in non-sedated, standing, or sternal patients. Barium, or a nonionic iodinated contrast agent, is administered in liquid form, mixed with gruel, and finally kibble with 3 to 5 swallows of each type.2 With cricopharyngeal achalasia, distention of the pharynx with food or liquid is followed by repeated pharyngeal contractions that result in only a small stream of contrast entering the esophagus.9

Picture 1 – A still photo from an esophagram of a dog with cricopharyngeal achalasia. Note the bolus of food in the pharynx and only small amount in the esophagus. There is no contrast present in the region of the cricopharyngeal muscle. It took multiple swallowing attempts for the bolus to pass through the UES.
Once cricopharyngeal achalasia is diagnosed, treatment is recommended. If the patient is hypothyroid, supplementation with L-thyroxine should be started.2,8 Temporary relief may be obtained with botulinum toxin A (BTA) injections into the cricopharyngeal muscle. The BTA weakens muscle contraction and has been used successfully in people with cricopharyngeal achalasia.12,13,14 The benefit of the BTA lasts for approximately four months in dogs, so it is not a permanent solution.15 If there is any question about the diagnosis, a positive response to BTA suggests that myectomy surgery would have a positive outcome. Suppose the patient does poorly following BTA injection. In that case, surgery may not be helpful, and reevaluating the diagnosis or looking for an underlying neuropathy is indicated. In people, surgery has a significantly higher success rate when compared to BTA injections.14 In dogs, surgical correction is recommended as it is the only option for permanent relief.3
Surgical treatment of cricopharyngeal achalasia involves myotomy or myectomy of the cricopharyngeus muscle.17 This can be performed through either a ventral or lateral approach.16,17 At Angell, we perform a myectomy via a lateral approach. A standard lateral approach to the larynx is performed, and an orogastric tube is passed to identify the muscle.17 The muscle is incised on its midline, and approximately 1 cm of muscle is removed.3,18 The thyropharyngeus muscle may also be incised to assure complete transection of the cricopharyngeus muscle.3 Failure to transect the entire cricopharyngeus muscle may result in continued clinical signs.17 The removed muscle should be submitted for histopathology.
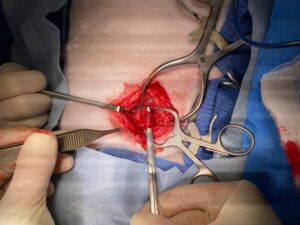
Picture 2 – Lateral approach to the cricopharyngeal muscle. The muscle is isolated prior to transection.
The surgery is typically performed unilaterally, although bilateral myectomy has been reported with success after unilateral surgery failed to alleviate the dysphagia.19 Postoperatively, patients are fed soft food or gruel for two days.3 They are then allowed to transition to their normal diet over several weeks slowly.3 Following myectomy, the resolution of dysphagia is immediate. However, temporary mild dysphagia may be due to swelling and discomfort at the surgery site.3 Dysphagia that continues more than several days is not expected and should be investigated. Incomplete myectomy or incorrect diagnosis are possible reasons for persistent dysphagia.17 Possible surgical complications include esophageal perforation, laryngeal paralysis, aspiration pneumonia, surgical site infection, and fibrosis at the surgery site resulting in recurrence of clinical signs.2,3,17 If the diagnosis is correct and the surgery performed successfully, the prognosis is excellent. If there is an underlying neuromuscular disease, the prognosis is more guarded. Careful case selection and full diagnostic testing are required to assure a successful outcome with surgery.
References
- Bingham DLC. Cricopharyngeal achalasia. Can Med Assoc J 1963; 89:1071-1073.
- Morrison JA, Mott J ed. Blackwell’s five-minute veterinary consult clinical companion: small animal gastrointestinal diseases. First ed. John Wiley & Sons, Inc. 2019; Chapter 27: 189-194.
- Elliott RC. An anatomic and clinical review of cricopharyngeal achalasia in the dog. JI S Afr Vet Assoc 2010; 81(2):75-9.
- Cook IJ. Cricopharyngeal function and dysfunction. Dysphagia 1993; 8:244-251.
- Weaver AD, Cricopharyngeal achalasia in cocker spaniels. J Small Anim Pract 1983; 24:209-214.
- Davidson AP, Pollard PE, Bannasch DL, et al. Inheritance of cricopharyngeal dysfunction in golden retrievers. AJVR 2004; 65(3):344-349.
- Peeters ME, Venker-van Haagen AJ, Goedegebuure SA, Wolvekamp WTC. Dysphagia in Bouviers associated with muscular dystrophy; evaluation of 24 cases. Vet Quart 1991; 23(2): 65-73.
- Bruchim Y, Kushnir A, Shamir MH. L-thyroxine responsive cricopharyngeal achalasia associated with hypothyroidism in a dog. J Sm Anim Pract 2005; 46:553-554.
- Pollard,RE. Imaging evaluation of dogs and cats with dysphagia. ISRN Vet Sci 2012Article ID 238505
- Pollard RE, Marks SL, Davidson A, Hornof WJ. Quantitative videofluoroscopic evaluation of pharyngeal function in the dog. Vet Rad Ultrasound 2000; 41(5): 409-412.
- Pollard RE, Marks SL, Cheney DM, Bonadio, CM. Diagnostic outcome of contrast videofluoroscopic swallowing studies in 216 dysphagic dogs. Vet Rad Ultrasound 2017; 1-8.
- Blitzer A, Brin MF. Use of botulinum toxin for diagnosis and management of cricopharyngeal achalasia. Otolaryngo Head Neck Surg 1997; 116:328-330.
- Messner A, Ho AS, Malhotra PS, et al. The use of botulinum toxin for pediatric cricopharyngeal achalasia. Int J Oed Otorhinolaryg 2011; 75:830-834.
- Kocdor P, Diegel ER, Tulunay-Ugar OE. Cricopharyngeal dysfunction: a systemic review comparing outcomes of dilatation, botulinum toxin injection, and myotomy. The Laryngosocpe 2016; 126:135-141.
- Marks SL. Rational approach to disorders of the canine esophagus: 15 years of experience. Proceedings ACVIM 2014.
- Papazoglou LG, Mann FA, Warnock, JJ, Song KJE. Cricopharyngeal dysphagia in dogs: the lateral approach for surgical management. Compendium 2006; 696-705.
- Warnock JJ, Marks SL, Pollard R, et al. Surgical management of cricopharyngeal dysphagia in dogs: 14 cases (1989-2001). JAVMA 2003; 223(10):1462-1468.
- Niles JD, Williams JM, Sullivan M, Crowsley FE. Resolution of dysphagia following cricopharyngeal myectomy in six young dogs. J Sm Anim Pract 2001; 42:32-35.
- Langlois DK, Stanley BJ, Ballegeer EA. Successful treatment of cricopharyngeal dysphagia with bilateral myectomy in a dog. Can Vet J 2014; 55:1167-1172.