-
Adopt
-
Veterinary Care
Services
Client Information
- What to Expect – Angell Boston
- Client Rights and Responsibilities
- Payments / Financial Assistance
- Pharmacy
- Client Policies
- Our Doctors
- Grief Support / Counseling
- Directions and Parking
- Helpful “How-to” Pet Care
Online Payments
Emergency: Boston
Emergency: Waltham
Poison Control Hotline
-
Programs & Resources
- Careers
-
Donate Now
 By Nicholas Trout, MA, VET MB, DACVS, ECVS
By Nicholas Trout, MA, VET MB, DACVS, ECVS
angell.org/surgery
surgery@angell.org
617-541-5048
In theory, there is no single way to correctly fix a fracture. So long as the surgeon adheres to the basic principles of orthopedics, fracture healing can occur just as effectively with an intramedullary pin and cerclage wires, as it can with a dynamic compression plate and screws. However, while open reduction and internal-fixation (ORIF) strives for anatomic reduction, it creates trauma through dissection, disturbance of the fracture hematoma, and interferes with the local blood supply. With subsequent concerns over non-union, osteomyelitis or implant failure, options for minimally invasive osteosynthesis (MIO) have increased in popularity and awareness. By decreasing surgical interference of the soft tissues and blood supply at a fracture site, fracture healing times can be reduced. Restoration of alignment becomes more important than precise anatomical reduction with an emphasis on construct stability to ensure early weight bearing. After decades of experience repairing human fractures, the use of minimally invasive nail osteosynthesis (MINO) can provide a meaningful alternative to popular plate and screw options to repair long bone fractures.
Fractures of the femur, tibia and humerus can lend themselves to repair with an interlocking nail system because they provide a nonarticular entry point for the nail. The nail is basically an intramedullary pin secured by locking bolts that capture the cis and trans cortex in the proximal and distal segments of the pin, thereby achieving axial bending strength together with torsional stability (figure 1). Biomechanically, fixation in the central axis is stronger than at the cortex, with respect to cyclic bending loads and fatigue failure.
In the absence of direct fracture visualization, preoperative radiographs of the fractures and contralateral (intact) limb provide vital information for planning. The size of nail can be determined, together with sites for bolt placement, and any problematic bone fissures noted, if they exist. Special markers on the radiographs offset problems with image magnification during this planning.
 Figure 1a) Plain radiograph, A/P view, of a mid-shaft tibia fracture in a skeletally mature dog. |
 Figure 1b) Post-operative A/P radiograph demonstrating repair with an interlocking nail. The nail was inserted just cranial to cranial cruciate ligament insertion in the proximal tibia, directed normograde, aiming for the talocrural joint. |
 Figure 1c) 26 days postoperative A/P radiograph of the healing fracture. (Figures 1 a, b and c courtesy of Biomedtrix) |
The I-Loc system (Biomedtrix) (figure 2) allows for normograde nail introduction without the need for power tools. Intramedullary insertion ensures that the periosteal blood supply is not disrupted. There is no need to contour a nail, as opposed to a bone plate. Insertion of the nail and placement of bolts only requires small, remote incisions. This system and jig design allows for accurate drilling and secure placement of locking bolts, avoids any mismatch of the holes between the nail and bolt, and negates the need for time-consuming and expensive fluoroscopy.
Most patients are weight bearing in 24-48 hours, interlocking nails offering a solid and secure fixation, particularly desirable in cases of polytrauma. Complete bone healing varies in time from 3-4 weeks to 10-12 weeks, depending on the age of the patient, concurrent disease, and nature/complexity of the underlying fracture. Initial restriction, use of physical therapy and incremental, structured increase in activity together with follow-up orthopedic and radiographic evaluations is similar to other fracture fixation techniques.
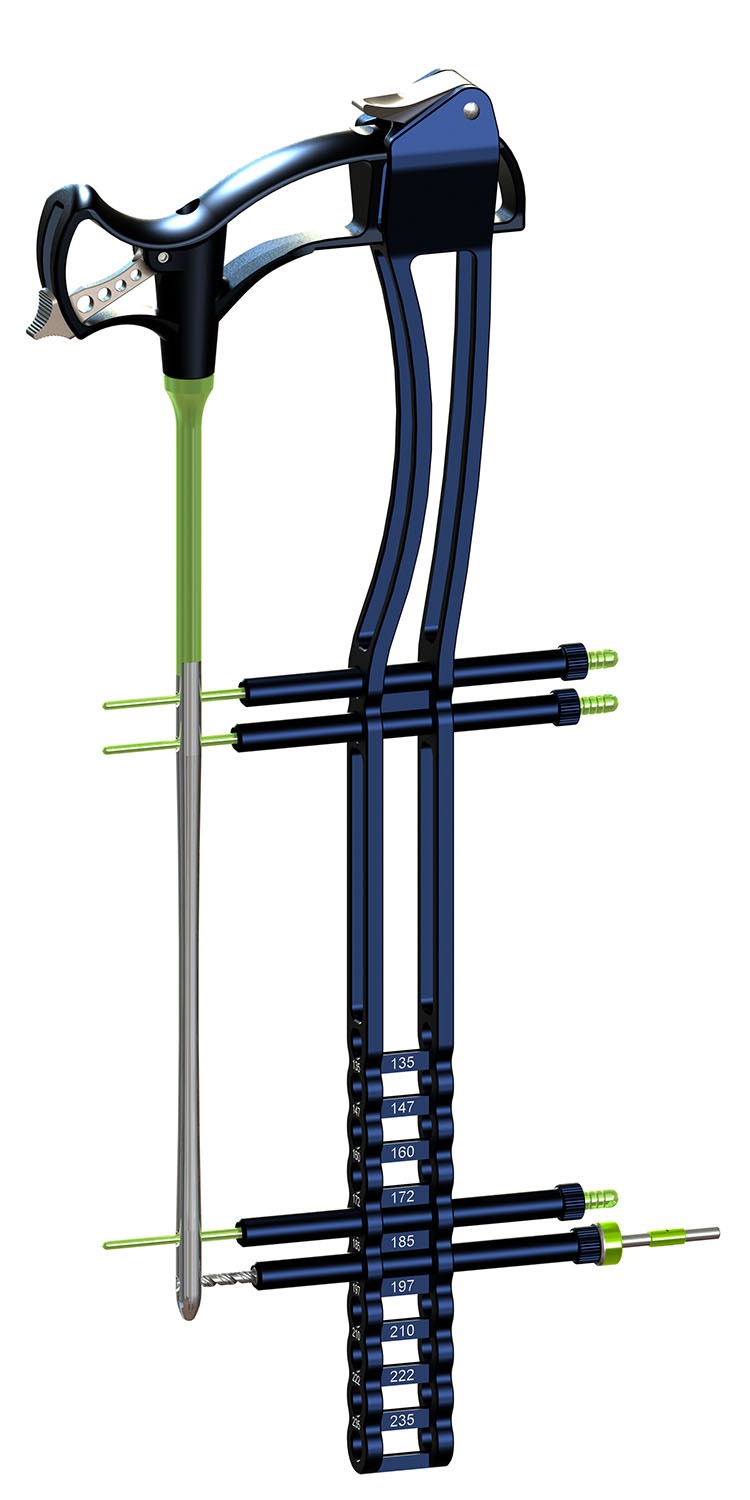
Figure 2: Biomedtrix I-Loc Interlocking Nail System (courtesy of Biomedtrix)
There are instances in which use of an interlocking nail should be avoided. In cases of open or infected fractures, non-union, or instances in which the fracture site needs to be directly visualized (removal of fibrous tissue, placement of cancellous bone graft), alternatives to interlocking nail fixation may be preferable.
References
Dejardin LM, Guiot LP, von Pfeil DJ. Interlocking nails and minimally invasive osteosynthesis. Vet Clin North Am Small Anim Pract 2012 Sep: 42 (5), 935-962.