-
Adopt
-
Veterinary Care
Services
Client Information
- What to Expect – Angell Boston
- Client Rights and Responsibilities
- Payments / Financial Assistance
- Pharmacy
- Client Policies
- Our Doctors
- Grief Support / Counseling
- Directions and Parking
- Helpful “How-to” Pet Care
Online Payments
Emergency: Boston
Emergency: Waltham
Poison Control Hotline
-
Programs & Resources
- Careers
-
Donate Now
 Michael M. Pavletic DVM, DACVS
Michael M. Pavletic DVM, DACVS
Director of Surgical Services
Angell Animal Medical Center
angell.org/surgery
617-541-5048
Introduction
Aural hematomas are the result of the rupture of the small vascular branches perforating the pinnal cartilage (scapha). Shearing forces are created from head shaking or blunt trauma to the pinna with blood pooling within the pinnal cartilage. This is contrary to previous reports that suggested that the hematoma forms between the medial pinnal skin and underlying perichondrium. As a result, the central scaphal cartilage partially separates or delaminates into medial and lateral “halves.”

Figure 1: Aural hematoma in a Vizsla, lateral aspect of the left pinna.
Contrary to the anatomy literature, anatomic dissection by the author revealed that the pinna (scapha) is not a solid sheet of cartilage: rather it is comprised of two adherent sheets of cartilage. The lateral sheet of cartilage is thinner than the medial sheet of cartilage comprising the scapha. During embryologic development, the pinna begins as a small triangular bud. As each bud enlarges and elongates, the lateral and medial layers contact and laminate together with connective tissue. The pinna assumes a flattened appearance as growth of the dog and cat continues. Small vascular channels perforate the conjoined layers, allowing small vessels originated from the lateral pinnal vasculature to supply the medial cartilage layer and overlying cutaneous surface.
Rupture of small perforating vessels is a result of a “stress-riser” effect, at the junction of the vessel and the semi-rigid pinnal cartilage. For example, violent head shaking or the ear striking a hard surface can cause a tear of one or more vessels. Blood escapes into the connective tissue gap between the medial and lateral cartilage layers, resulting in aural hematoma formation.
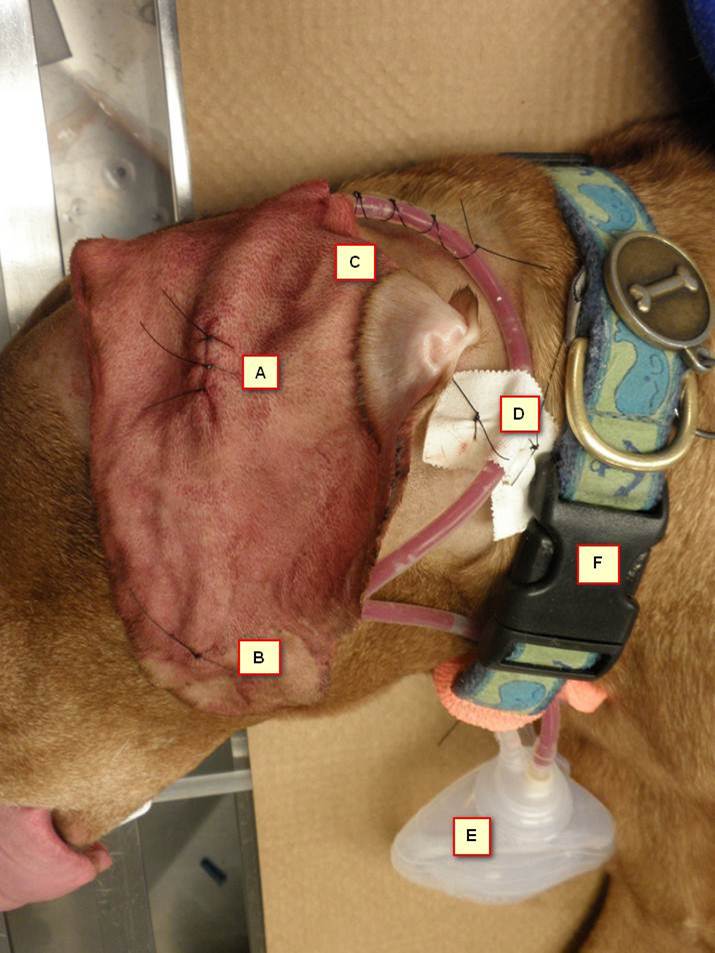
Figure 2: Vacuum Drain System. “A” indicates the accession incision for drain placement, lateral aspect of the pinna. (B) After trimming the length of the fenestrated component of the drain tubing to accommodate the length of the hematoma cavity, a single suture is used to secure the tip of the drain through the skin surface. (C) After trimming the non-fenestrated portion of the vacuum drain to reach the future location of the vacuum reservoir, a stab incision is created at the base of the pinna. Forceps are then used to bluntly dissect to the initial access incision where the end of the non-fenestrated drain section is grasped and retracted out of the stab incision. A purse-string suture and finger trap knot secure the drain to this stab incision. (D) A strip of one inch surgical tape is secured to the exit drain and is, in turn, sutured to the lateral cervical skin to prevent displacement of the drain in each tape tab. (E) The drain is secured to the Jackson-Pratt vacuum reservoir. (F) The patient’s dog collar is threaded through the plastic loop on the Jackson-Pratt reservoir. The vacuum reservoir is activated, providing continuous suction to collapse the hematoma cavity.
There are a variety of medical and surgical treatments advocated in managing aural hematomas, including:
- Intralesional and systemic corticosterioid therapy.
- Aspiration followed by compression bandages.
- No treatment.
- Passive drains (Larson’s teat cannulas, Penrose drains, fenestrated tubing)
- Vacutainer Drainage Technique (Modifying a butterfly catheter as a drain attached to a Vacutainer Glass Collection Tube.)
- Incisional drainage followed by “Though and Through” Pinnal Sutures.
- Fenestration of the medial pinnal surface.
To date, drainage of aural hematomas is considered the best option for their management, although the results between techniques are variable. All drainage technics previously described involved the concave/medial surface of the pinna. A bandage is normally required with these drainage techniques to protect the affected pinna until healing is complete. [The primary goal is to support fibrous connective tissue to reattach the compressed pinnal cartilage surfaces back together while simultaneous drainage prevents a fluid pocket from reforming.] Incisional drainage (linear, sigmoid) followed by suture placement is the most commonly employed procedure in small animal surgery.

Figure 3: Postoperative view of the medial aspect of the pinna. The arrows denote the silhouette of the drain after the activated drain removes the fluid contents of the aural hematoma.
Complications seen with aural hematoma management include: a.) recurrent hematoma formation secondary to re-injury, insufficient drainage or incomplete healing; b.) permanent pinnal thickening and wrinkling/deformity of the ear secondary to fibrosis and contracture; c.) obstruction or premature displacement of drain tubes; d.) delayed incisional healing; and e.) problematic bandage application/maintenance to protect and immobilize the affected ear, while providing local access to the drainage site. Unruly dogs also may require the adjunctive use on an Elizabethean collar to prevent repetitive pawing. The cost associated with open wound care and periodic bandage changes can be cumulatively expensive.
The author developed the use of a vacuum drain system to manage aural hematomas in the dog and cat by placement of the drain on the convex/lateral surface of the pinna. This minimally invasive technique is remarkably effective in managing aural hematomas. Protected by an Elizabethean collar, no bandage is required.
Laterally Placed Vacuum Drain Technique in 10 Steps (SEE Figures 1-4)
- Both sides of the involved pinna are clipped of fur, including the base of the ear and adjacent cervical skin. The skin is prepared for surgery and draped.
- A 1cm skin incision is created on the lateral/convex skin surface below the base of the aural hematoma with a No. 15 scalpel blade. Care is taken to avoid incising major branches of the auricular vessels.
- A No. 11 scalpel blade is directed through the skin incision and into the base of the cartilage-encased hematoma cavity using a quick stabbing motion. The blade is withdrawn and a mosquito hemostat is introduced into the hematoma incision to facilitate fluid evacuation.
- The fenestrated portion of a Hemaduct vacuum drain (Jackson-Pratt Hemaduct Round Drain, Cardinal Healthy, McGaw Park, IL [10Fr, 15Fr, 19Fr]) is shorted with scissors to traverse the hematoma cavity. The drain is inserted along the length of the hematoma. A single 3-0 suture is placed through the overlying skin, with the suture needle inserted through the center of the palpable drain tip before exiting the skin.
- The non-fenestrated portion of the drain is measured so that it can reach the lower vacuum reservoir that will be secured to the patient’s cervical collar. Excessive drain is then cut off with scissors.
- A smaller stab incision is made in the cervical skin adjacent to the base of the pinna. Metzenbaum scissors or a hemostat can be used to blunt dissect a narrow subcutaneous tunnel between the two skin incisions.
- A hemostat is then introduced through the stab incision with its tip exiting the initial pinnal incision. The free end of the drain is then grasped and retracted out of the stab incision.
- The pinnal skin incision is closed with two or three interrupted 3-0 skin sutures. The pinna is gently manipulated to assure the drain is under no tension during normal movement of the pinna.
- A 2-0 nylon purse-string suture is placed around the cutaneous stab incision and a “finger trap” knot used to secure the non-fenestrated portion of the drain exiting the skin. A short strip of surgical tape is applied to the drain, approximately 5 cm from the cutaneous exit site of the drain: two sutures are placed through the tape tabs created on each side of the drain to minimize the risk of accidental drain displacement.
- The drain is connected to reservoir and the vacuum is activated. The vacuum reservoir is attached to the patient’s dog collar. An Elizabethean Collar is applied to the dog.

Figure 4: The patient at Day 18 for drain removal. After removal of the sutures, the drain slides out of the pinna and is discarded along with the vacuum reservoir. This minimally invasive approach to aural hematomas reduces surgical trauma and deformity of the pinna secondary to scar tissue. Cosmetic results have been remarkably good when this system is used early in the course of hematoma formation and subsequent management.
Patients are normally placed on Clavamox (Pfizer Animal Health, NY, NY) or another broad-spectrum antibiotic and discharged on pain medication for one week. Topical ointment may be used to treat any underlying otitis externa. Owners are instructed on the use of the vacuum drain system; they recorded the daily volume of fluid retained in the reservoir. (This normally amounts to < 2ml/day.) The patient can be rechecked on a weekly basis to assure the drain is functional and healing was progressing. The drain and skin sutures are subsequently removed in 18-21 days after their placement. The Elizabethean Collar can be applied for an additional week if the veterinarian has concerns over the patient disturbing the ear.
Comments
Both dogs and cats tolerate the drainage system and owners found emptying the reservoir simple to perform. The owners record the volume of the fluid on a daily basis, which helps the veterinarian to determine when the drain can be removed. This minimally invasive approach is less traumatic and painful compared to the use of the conventional incisional drainage/ suture approach. With a little practice, the technique is notably faster and easier to perform compared to incisional drainage/suturing. Additionally, no bandage is required, reducing the cost to the owner. Having the drain exit at the lateral base of the pinna better protects it from displacement, in conjunction with the Elizabethean collar.
Scarring is minimized with this technique whereas conventional incisional drainage procedure normally causes significant pinnal distortion /wrinkling secondary to greater scar tissue deposition and contracture. When managed early after hematoma development, the cosmetic results with the vacuum drain technique are often excellent in dogs.
From my studies to date, it has been noted that [in the occasional dog and most cats] the thinner lateral pinnal cartilage layer can stretch from pressure generated by the expanding hematoma: this asymmetrical stretching of the lateral cartilage layer creates a small redundant fold of tissue when it is drawn against the flat medial cartilage layer upon activation of the vacuum reservoir. .The thicker medial pinnal layer, reinforced by the close adherence of the skin to its perichondrial surface, prevents significant deformation from the pressure exerted by the expanding hematoma. Long standing hematomas are prone to deforming the pinna from chronic inflammation resulting in additional connective tissue deposition. Early intervention using this drainage technique has the best chance to resolve aural hematomas with better cosmetic results.
[Readers are welcome to contact me if you have any questions regarding this drainage option for aural hematomas.]
Reference: Pavletic MM. (2015) Use of laterally placed vacuum drains for management of aural hematomas in five dogs. J Am Vet Med Assoc 246:112-117.