-
Adopt
-
Veterinary Care
Services
Client Information
- What to Expect – Angell Boston
- Client Rights and Responsibilities
- Payments / Financial Assistance
- Pharmacy
- Client Policies
- Our Doctors
- Grief Support / Counseling
- Directions and Parking
- Helpful “How-to” Pet Care
Online Payments
Emergency: Boston
Emergency: Waltham
Poison Control Hotline
-
Programs & Resources
- Careers
-
Donate Now
 Nick Trout, MA, VET MB, DACVS, ECVS
Nick Trout, MA, VET MB, DACVS, ECVS
angell.org/surgery
surgery@angell.org
617-541-5048
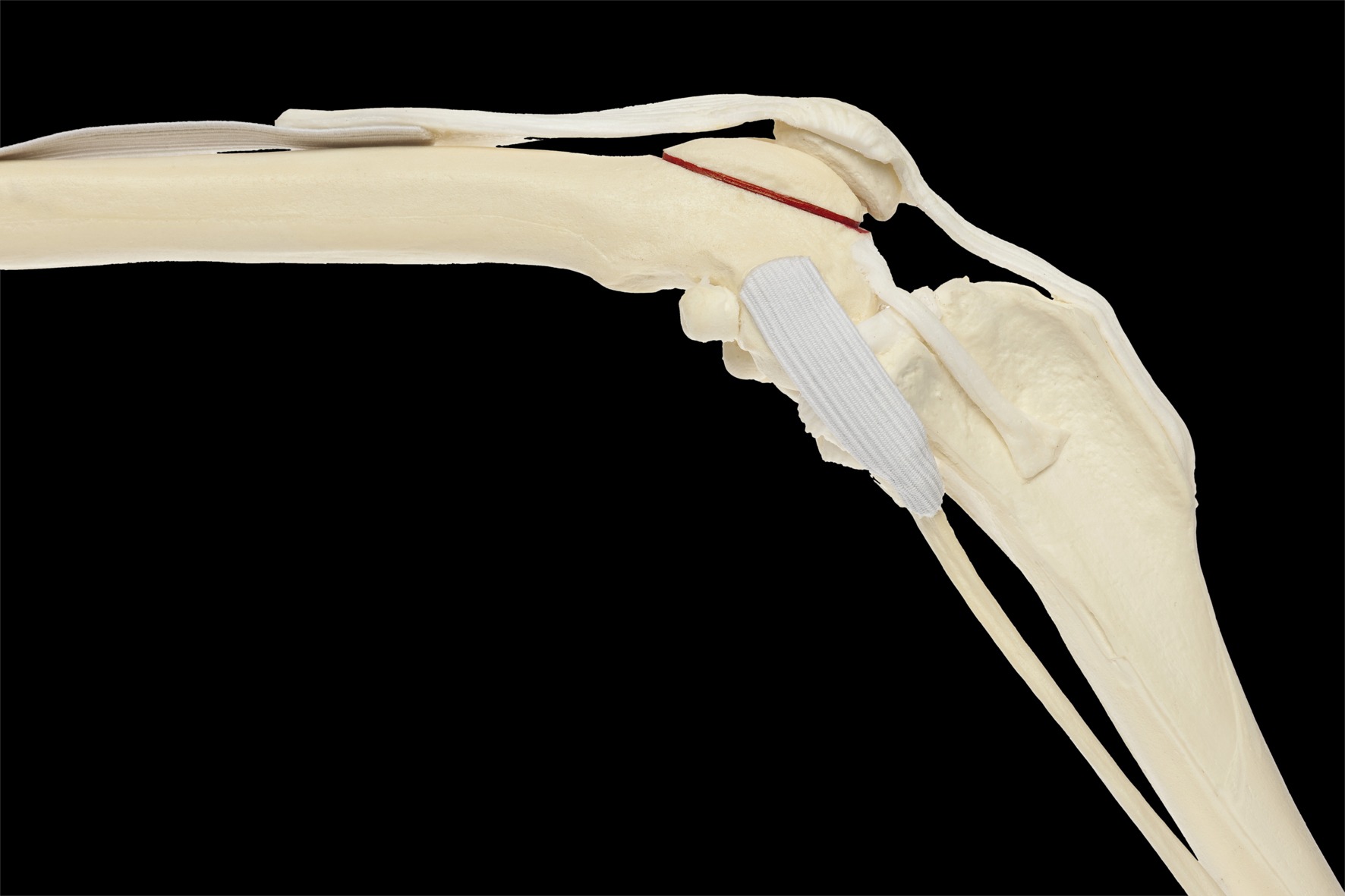
Figure 1. Bone model, lateral position, red-inked line delineating the axis of a required osteotomy from the origin of the long digital extensor tendon to the proximal margin of the trochlear groove.
Canine patellar luxation is an extremely common orthopedic condition that, at the time of corrective surgery, necessitates evaluation of the patellar groove with respect to alignment, depth, shape, and cartilage quality. For the most part, groove abnormalities can be addressed with either a wedge recession or block trochleaplasty, however, there are occasions in which the patella groove is so severely deformed or damaged that the surgeon is forced to perform a sulcoplasty, burring or rasping away what cartilage exists to expose bleeding subchondral bone in order to create a ‘faux’ groove to ‘capture’ the patella. Sulcoplasty is painful, results in a slower return to function, and, compared to trochleaplasty, ensures sub-optimal development of fibro-cartilage over a larger surface area.
An appropriately sized, anatomically shaped, low friction prosthesis, Patellar Groove Replacement (PGR, KYON) offers the surgeon an alternative to sulcoplasty in cases of severe femoro-patellar osteoarthritis. Dogs should be greater than six months of age and trochlear deformities can be addressed secondary to either lateral or medial patellar luxation. Careful preoperative radiographic planning is essential in order to choose the correct size of prosthesis.
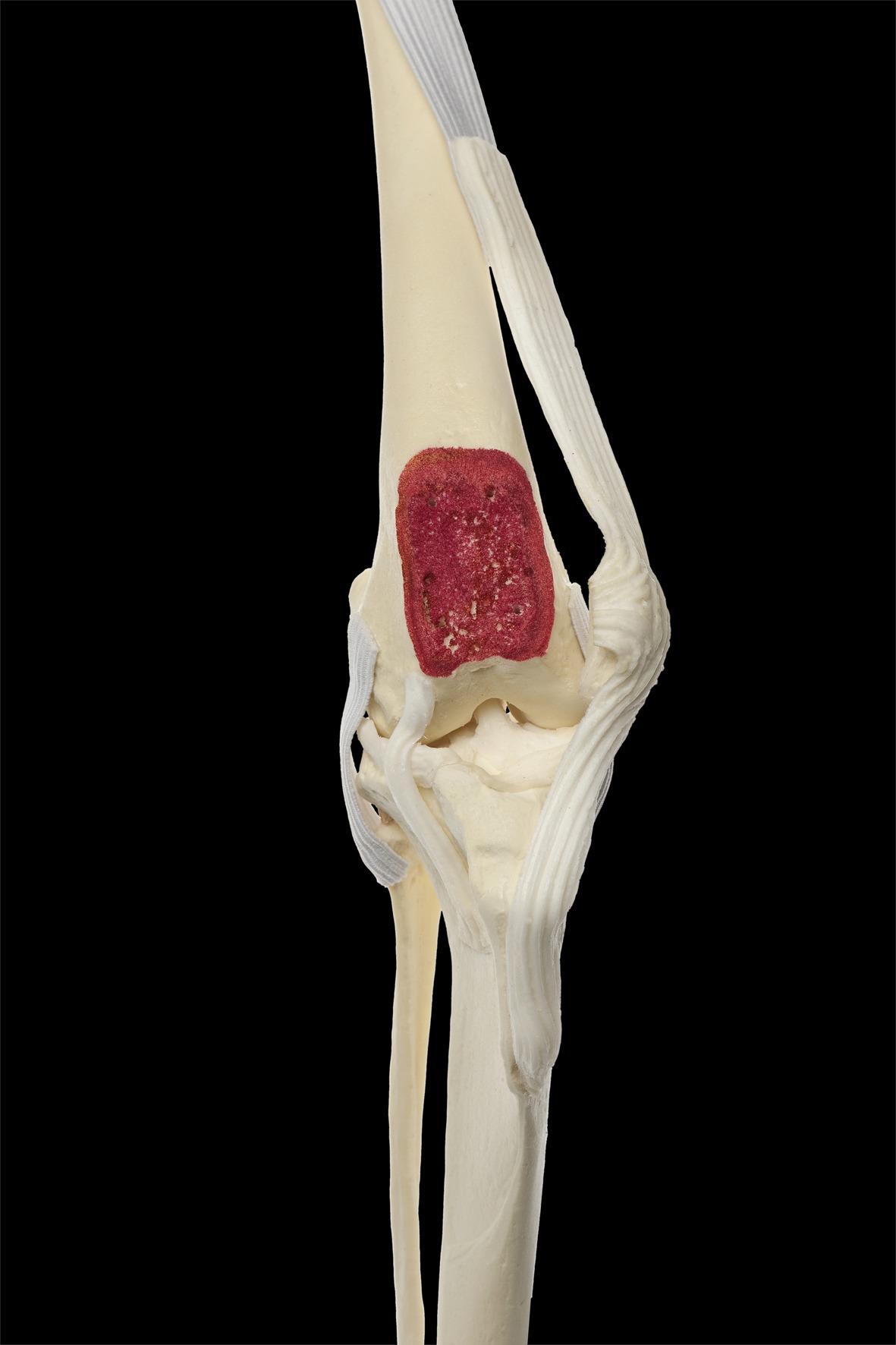
Figure 2. Bone mode, A/P position, representing the appearance of a smooth flat bone surface required for bone plate application.
The stifle joint is approached routinely, the patella luxated and the groove exposed. An osteotomy to remove the diseased groove is performed using an oscillating saw along a line from the origin of the long digital extensor tendon to the proximal margin of the trochlear groove (figure 1). This will leave a flat, smooth, bony bed (figure 2) on which to secure an implant base plate (figure 3). Screws secure the plate in the appropriate position. The prosthesis has three prongs that engage the plate before being carefully and gently hammered into the locked position (figures 4 & 5). Prior to final prosthesis choice and placement, use of trial implants, together with patella reduction and stifle flexion/extension, is vital to ensure the correct size, a ‘snug’ relationship between patella and implant, smooth tracking, and absence of a click or hitch as the patella glides.
It is important to note that the PGR is not, in itself, a cure for patella luxation. All the other standard concurrent treatments—joint capsule release/imbrication, tibial tuberosity transposition, distal femoral or proximal tibial corrective osteotomies—are still essential to a positive outcome.
One of the advantages to PGR over sulcoplasty is the lack of innervation to a prosthesis, owners noting increased comfort and earlier return to function. Kyon suggests a two-week period of postoperative restriction, introduction of five-minute leash walks at week three and return to normal by weeks eight to ten. Radiographic follow up to ensure stable implants can be useful at this time, however bone ingrowth into the base plate has been reported to take nine months.

Figure 3 (top left): Base plate screwed into the appropriate position. Figure 4 (top right): Bone model, A/P position, demonstrating PGR (patella luxated). Figure 5 (bottom): Bone model, lateral position, demonstrating PGR (patella reduced).
Reference:
- Patellar groove replacement in patellar luxation with severe femoro-patellar osteoarthritis. Z. Dokic, D. Lorinson, JP Weigel, A Vezzoni. Vet Comp Orthop Traumatol 2/2015; 124-130.
- All figures are courtesy of KYON(www.kyon.ch)