-
Adopt
-
Veterinary Care
Services
Client Information
- What to Expect – Angell Boston
- Client Rights and Responsibilities
- Payments / Financial Assistance
- Pharmacy
- Client Policies
- Our Doctors
- Grief Support / Counseling
- Directions and Parking
- Helpful “How-to” Pet Care
Online Payments
Emergency: Boston
Emergency: Waltham
Poison Control Hotline
-
Programs & Resources
- Careers
-
Donate Now
 Nick Trout, MA, VET MB, DACVS, ECVS
Nick Trout, MA, VET MB, DACVS, ECVS
www.angell.org/surgery
surgery@angell.org
617-541-5048
Perhaps it reflects breed popularity (Golden retrievers, Labradors, Bernese mountain dogs, Rottweilers), but at Angell the dominant subtypes of canine elbow dysplasia are fragmented medial coronoid process (FMCP) and osteochondritis dissecans (OCD). FMCP is a separation of the medial aspect of the coronoid process from the ulna whereas OCD is caused by failure of normal endochondral ossification on the medial aspect of the humerus. The long term effect of these developmental imperfections is degenerative joint disease (DJD) leading to wear and erosion of cartilage on the medial aspect of the elbow joint. When visualized arthroscopically (Figure 1) the delineation between destroyed cartilage medially and healthy white pristine cartilage in the lateral compartment is striking.
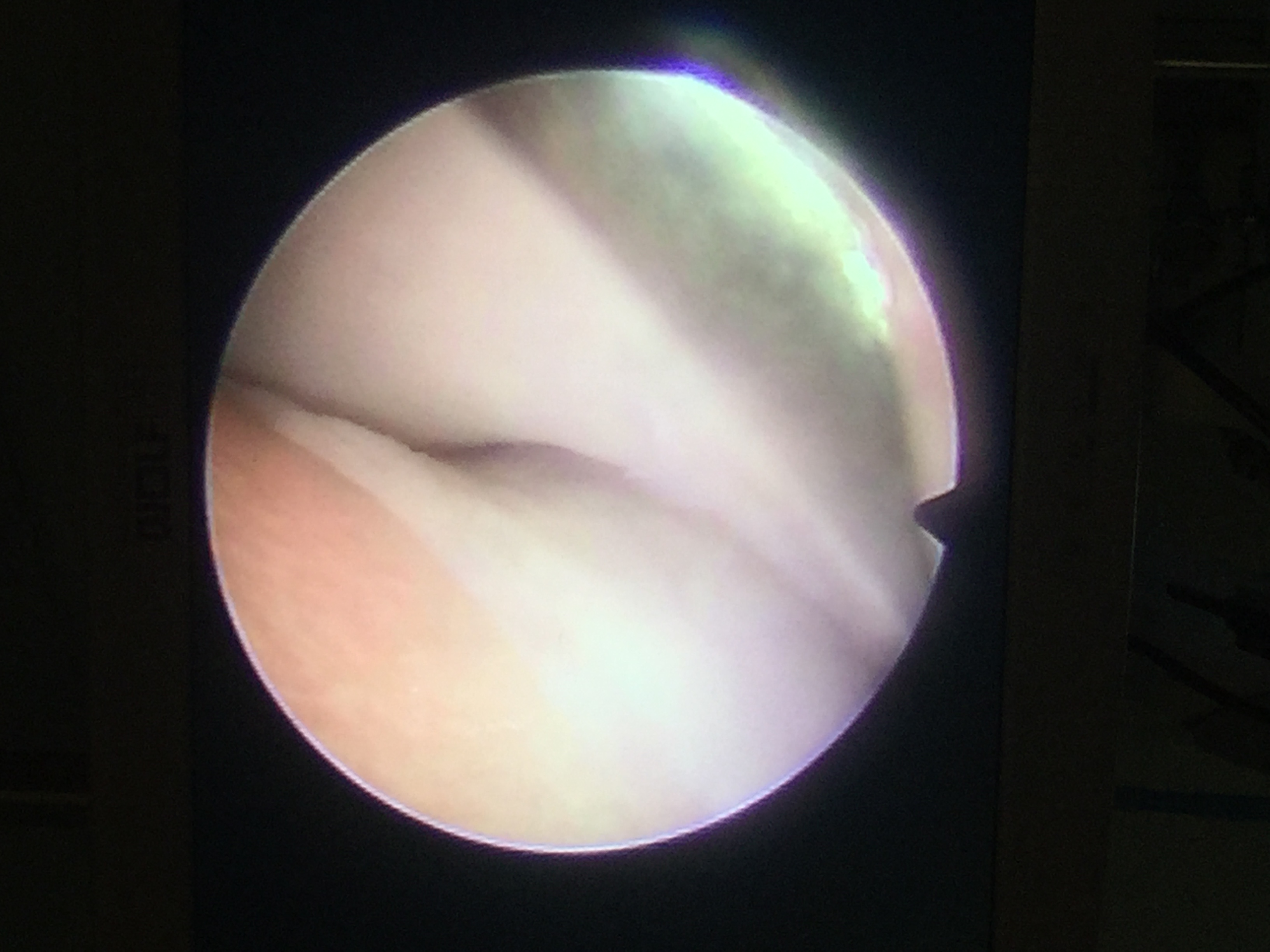
Figure 1: Arthroscopic image of an elbow joint documenting delineation between eroded cartilage in the medial compartment and more normal cartilage in the lateral compartment
Biomechanical studies have suggested that dogs load about 65% on the medial aspect of the elbow joint, and 35% on the lateral aspect. What if it were possible to make a subtle change in limb alignment that would unload the medial compartment, make better use of that healthy lateral cartilage and in doing so reduce pain and improve elbow function? This is, in broad terms, the general premise behind PAUL, the proximal abducting ulna osteotomy (Kyon Veterinary Surgical Products).
Pendo, a five year old neutered male Golden retriever had been medically managed for DJD secondary to left elbow dysplasia for many years. More recently his function had been declining despite excellent weight management, exercise limitations, joint supplements and meloxicam. Pendo appeared to be a good candidate for a PAUL procedure. Following radiographic preoperative planning, the affected elbow was scoped to ensure cartilage damage was limited to the medial compartment and, in Pendo’s case, to remove a loose coronoid fragment. The caudal approach to the proximal ulna is simple, with minimal soft tissue dissection, allowing an ulna osteotomy with an oscillating saw to create a small caudal step of two to three millimeters in the proximal ulna, lowering the coronoid. This is secured using a titanium six-hole, PAUL plate (Kyon) applied to the lateral aspect of the ulna, spanning the osteotomy gap (Figures 2 and 3).

Lateral view (figure 2) and a caudo-medial cranio-lateral oblique view (figure 3) of a bone model to demonstrate ulna osteotomy and PAUL plate application (images courtesy of Kyon www.kyon.ch)

Figure 3
Postoperative radiographs confirmed appropriate implant position (Figures 4 and 5) and the leg was placed in a soft padded bandage for one to two weeks. Exercise restriction is important for the next 6-8 weeks but physical therapy, including hydrotherapy, can begin at week four.

Lateral (figure 4) and AP (figure 5) postoperative radiographs of Pendo’s radius/ulna. Note the significant degenerative joint disease in the elbow.

Figure 5
The ulna is often slow to heal and the majority of dogs will take at least 3-6 months to see maximal clinical improvement. In Pendo’s case his lameness was better than before surgery in just a few weeks. Nine months later he was going for 45 minute leash walks twice daily, playing off leash and limping the day after higher levels of activity, things that he was been unable to do for years.
I am assured that a large multi-center study of PAUL cases and their outcomes is in the works. For now we are forced to rely upon smaller case numbers. One study (R. Whitelock; PAUL Clinical Experience Symposium Presentation, 2014), involving 32 cases, asked owners whose dogs had undergone PAUL, “How is your dog now compared to pre-surgery?” None said “worse,” one said “same” and 31/32 said “better.” Seventy-two percent noted some degree of lameness during certain activities, but ninety-seven percent reported meaningful improvement.
Pendo may be my poster dog for PAUL, and I am always wary of anecdotes as proof of success, however, PAUL does appear to have a place as a viable treatment alternative in carefully selected cases where clinicians and owners are frustrated by the challenges of medical management for chronic elbow dysplasia.
For more information about Angell’s Surgery service, please visitwww.angell.org/surgery. Dr. Trout can be reached at 617-541-5048, or by e-mailing surgery@angell.org.