-
Adopt
-
Veterinary Care
Services
Client Information
- What to Expect – Angell Boston
- Client Rights and Responsibilities
- Payments / Financial Assistance
- Pharmacy
- Client Policies
- Our Doctors
- Grief Support / Counseling
- Directions and Parking
- Helpful “How-to” Pet Care
Online Payments
Emergency: Boston
Emergency: Waltham
Poison Control Hotline
-
Programs & Resources
- Careers
-
Donate Now
 by Sue Casale, DVM, DACVS
by Sue Casale, DVM, DACVS
Angell Animal Medical Center
617-541-5048
surgery@angell.org
Liver lobectomies are performed for a variety of reasons in companion animals and are one of the most common hepatic procedures performed in veterinary medicine. Neoplasia, lobe torsion, cysts and abscesses may all require partial or complete removal of a liver lobe. Although fairly simple to perform, multiple complications associated with this procedure have been reported. The most common major complication following liver lobectomy is hemorrhage, which can often be life threatening.1 Intraoperative hemorrhage has been reported in 25% of patients undergoing liver lobectomy, with major hemorrhage in over 7% of those patients.2 Multiple factors can increase the risk of hemorrhage. Patients undergoing hepatic surgery often have systemic illness with up to 93% of dogs and 82% of cats with liver disease having abnormalities in their coagulation profile.1 Liver anatomy can also make surgery challenging. The portal vein branches, which supply a majority of the hepatic blood, are thin-walled and prone to hemorrhage with dissection.1 The lobes in the right division of the liver are adhered to the caudal vena cava making removal difficult, or in some cases, impossible. Another complicating factor is that many liver tumors are very large. The most common liver tumor in dogs is hepatocellular carcinoma (HCC) with 61% of cases of the massive subtype.2 Because this subtype is typically present in a single lobe, surgical resection is recommended because even with incomplete margins, low recurrence and distant metastasis rates are reported.2
 Reported techniques for liver lobectomy include blunt dissection and vessel ligation, use of TA autostaplers, vessel sealing devices, harmonic scalpels and encircling suture ligatures such as the commercially available self-ligating loop (SLL).3,4,5 A comparison of these techniques has shown no significant difference in overall surgical time but significantly more blood loss was seen with the blunt dissection technique.4 The SLL has been shown to be the technique most resistant to leakage in a postmortem study comparing these five techniques.6 This, combined with the ease of use and low cost of the SLL (about 1/3 the cost of an autostapler), make its use in veterinary medicine especially appealing. The SLL consist of suture with a sliding (Roeder) knot that when tightened, locks and maintains the security of the ligature.7 The SLL was originally designed for use in minimally invasive procedures such as laparoscopy or thoracoscopy. The suture is encased in a nylon knot-pushing device that allows for simplicity of application even in tight areas. When tightened on the hepatic parenchyma, the suture partially cuts through the parenchyma and crushes the larger vessels and biliary ducts. Parenchyma distal to the SLL is excised leaving a 2-3mm cuff of tissue to decrease the risk of ligature slippage.4
Reported techniques for liver lobectomy include blunt dissection and vessel ligation, use of TA autostaplers, vessel sealing devices, harmonic scalpels and encircling suture ligatures such as the commercially available self-ligating loop (SLL).3,4,5 A comparison of these techniques has shown no significant difference in overall surgical time but significantly more blood loss was seen with the blunt dissection technique.4 The SLL has been shown to be the technique most resistant to leakage in a postmortem study comparing these five techniques.6 This, combined with the ease of use and low cost of the SLL (about 1/3 the cost of an autostapler), make its use in veterinary medicine especially appealing. The SLL consist of suture with a sliding (Roeder) knot that when tightened, locks and maintains the security of the ligature.7 The SLL was originally designed for use in minimally invasive procedures such as laparoscopy or thoracoscopy. The suture is encased in a nylon knot-pushing device that allows for simplicity of application even in tight areas. When tightened on the hepatic parenchyma, the suture partially cuts through the parenchyma and crushes the larger vessels and biliary ducts. Parenchyma distal to the SLL is excised leaving a 2-3mm cuff of tissue to decrease the risk of ligature slippage.4
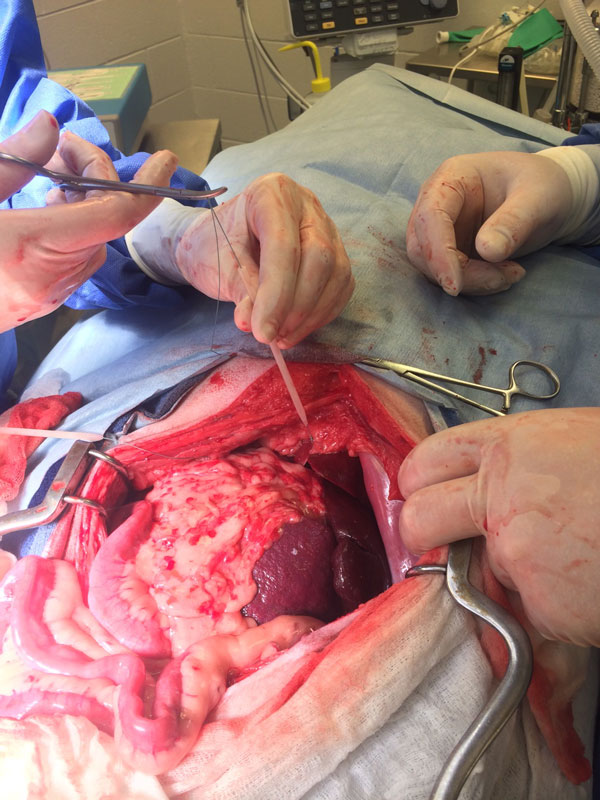 The SLL has been used successfully for over 5 years at Angell Animal Medical Center on a variety of companion animals including dogs, cats, rabbits and ferrets. We have recently reported the results of 32 liver lobectomies performed with the SLL and well as a modification of the SLL device to allow application in a variety of cases.3 In our report, intraoperative hemorrhage was encountered in only 12.5% of cases. All were successfully managed at the time of surgery and none were considered major. Only one patient, that had two liver lobes removed, developed a hemoabdomen post-operatively which was successfully managed conservatively. Ninety –seven percent of patients were discharged from the hospital. Although a single SLL was tested in the previous postmortem study, in most cases at Angell, two SLLs were used.6 A second SLL is easily applied and may allow for extra security, especially when large masses are removed. Application of the second SLL on top of the first also allows alternating tightening of the SLL to ensure complete ligation of the vessels. Hemorrhage (intraoperative or postoperative) was not noted in any case where more than one SLL was applied. One previously reported disadvantage of the SLL is the size of the ligature.4 The median volume of massive HCC has been previously reported as 1,320 cm.3,4 As commercially available, the diameter of the SLL is 8cm which makes application to these larger masses impossible. Expansion of the SLL can be achieved by shortening the application device and pulling the suture proximally through the slipknot. To shorten the device, we use a pin cutter to cut through the plastic applicator while avoiding cutting the suture. With this technique, the loop can be expanded up to 15 cm, allowing successful application to very large liver masses. Because of the low cost, ease of use and success with limiting intraoperative hemorrhage, the SLL has become our preferred method of liver lobectomy at Angell.
The SLL has been used successfully for over 5 years at Angell Animal Medical Center on a variety of companion animals including dogs, cats, rabbits and ferrets. We have recently reported the results of 32 liver lobectomies performed with the SLL and well as a modification of the SLL device to allow application in a variety of cases.3 In our report, intraoperative hemorrhage was encountered in only 12.5% of cases. All were successfully managed at the time of surgery and none were considered major. Only one patient, that had two liver lobes removed, developed a hemoabdomen post-operatively which was successfully managed conservatively. Ninety –seven percent of patients were discharged from the hospital. Although a single SLL was tested in the previous postmortem study, in most cases at Angell, two SLLs were used.6 A second SLL is easily applied and may allow for extra security, especially when large masses are removed. Application of the second SLL on top of the first also allows alternating tightening of the SLL to ensure complete ligation of the vessels. Hemorrhage (intraoperative or postoperative) was not noted in any case where more than one SLL was applied. One previously reported disadvantage of the SLL is the size of the ligature.4 The median volume of massive HCC has been previously reported as 1,320 cm.3,4 As commercially available, the diameter of the SLL is 8cm which makes application to these larger masses impossible. Expansion of the SLL can be achieved by shortening the application device and pulling the suture proximally through the slipknot. To shorten the device, we use a pin cutter to cut through the plastic applicator while avoiding cutting the suture. With this technique, the loop can be expanded up to 15 cm, allowing successful application to very large liver masses. Because of the low cost, ease of use and success with limiting intraoperative hemorrhage, the SLL has become our preferred method of liver lobectomy at Angell.
For more information about Angell’s Surgery service, please visit www.angell.org/surgery. Dr. Casale can be reached at 617-541-5048, or by e-mailing scasale@angell.org or surgery@angell.org.
References:
- May LR, Mehler SJ. Complications of hepatic surgery in companion animals. Vet Clin North Am Small Animal Pract 2011; 41:935-948.
- Liptak JM, Dernell WS, Monnet E, et al. Massive hepatocellular carcinoma in dogs: 48 cases (1992-2002). J Am Vet Med Assoc 2004; 225:1225-1230.
- Goodman AR, Casale SA. Short-term outcome following partial or complete liver lobectomy with a commercially prepared self-ligating loop in companion animals: 29 cases (209-2012). J Am Vet Med Assoc 2014; 244:693-698.
- Risselada M, Ellison GW, Bacon NJ, et al. Comparison of 5 surgical techniques for partial liver lobectomy in the dog for intraoperative blood loss and surgical time. Vet Surg 2010; 39: 856-862.
- Lewis DD, Bellenger CR, Lewis DT, et al. Hepatic lobectomy in the dog: A comparison of stapling and ligation techniques. Vet Surg 1990; 19:221-225.
- Risselada M, Poluak MM, Ellison GW, et al. Postmortem evaluation of surgery site leakage by use of in situ isolated pulsatile perfusion after partial liver lobectomy in dogs. Am J Vet Res 2010; 71:262-267.
- Cuddy LC, Risselada M, Ellison GW. Clinical evaluation of a pre-tied ligating loop for liver biopsy and liver lobectomy. J Small Anim Pract 2013; 54:61-66.