-
Adopt
-
Veterinary Care
Services
Client Information
- What to Expect – Angell Boston
- Client Rights and Responsibilities
- Payments / Financial Assistance
- Pharmacy
- Client Policies
- Our Doctors
- Grief Support / Counseling
- Directions and Parking
- Helpful “How-to” Pet Care
Online Payments
Emergency: Boston
Emergency: Waltham
Poison Control Hotline
-
Programs & Resources
- Careers
-
Donate Now
By Terry Huh, DVM, DACVIM (Cardiology)![]()
angell.org/cardiology
cardiology@angell.org
617-541-5038
March 2024
x
x
x
Introduction
Cardiac disease is a common cause of morbidity and mortality in dogs and cats. Focused cardiac ultrasound (FCU) is a tool that allows one to identify certain ultrasonographic features of heart disease, such as chamber enlargement, cavitary effusions, or systolic dysfunction, which can ultimately help guide clinical decision-making, typically in an emergency setting. FCU, as defined by the American Society of Echocardiography, refers to a “focused examination of the cardiovascular system performed by an appropriately trained clinician (typically not a cardiologist) by using ultrasound as an adjunct to the physical examination to recognize specific ultrasonic signs that represent a narrow list of potential diagnoses in specific clinical settings.” FCU findings should not be used in isolation but rather be interpreted in conjunction with the patient’s signalment, history, physical examination findings, and other imaging modalities, namely thoracic radiography.
This article highlights some of the more common clinical indications of FCU in small animal practice. The interested reader is encouraged to peruse the review articles cited under references for further information. While there are no available guidelines that outline specific training needed to perform FCU proficiently, there is a growing body of resources and hands-on training opportunities through continuing education courses that can help improve the confidence and accuracy of FCU.
Clinical Indication 1: The Dyspneic Cat
 Treating the dyspneic feline patient is challenging. Obtaining thoracic radiographs on presentation can be difficult due to the fragile nature of these patients, and the clinician is often faced with the difficult task of deciding how to stabilize the patient with minimal information. FCU can help differentiate cardiac vs. non-cardiac causes of dyspnea and has several advantages in this setting. It can be performed rapidly with portable equipment and typically does not require significant restraint. FCU can also be easily incorporated into other point-of-care ultrasound assessments, namely thoracic and abdominal focused assessment with sonography for trauma, triage, and tracking (TFAST and AFAST), as well as veterinary bedside lung ultrasound exam (Vet BLUE).
Treating the dyspneic feline patient is challenging. Obtaining thoracic radiographs on presentation can be difficult due to the fragile nature of these patients, and the clinician is often faced with the difficult task of deciding how to stabilize the patient with minimal information. FCU can help differentiate cardiac vs. non-cardiac causes of dyspnea and has several advantages in this setting. It can be performed rapidly with portable equipment and typically does not require significant restraint. FCU can also be easily incorporated into other point-of-care ultrasound assessments, namely thoracic and abdominal focused assessment with sonography for trauma, triage, and tracking (TFAST and AFAST), as well as veterinary bedside lung ultrasound exam (Vet BLUE).
For example, identification of an enlarged left atrium to aorta (LA/Ao) ratio of 2:1, in conjunction with B-line artifacts on Vet BLUE lung ultrasound (which can support the presence of pulmonary edema) as well as the presence of pleural and/or pericardial effusion, would dramatically increase the suspicion of congestive heart failure, and prompt the clinician to administer a furosemide bolus as the first step in stabilizing the patient. The author reminds the reader that such a patient should ultimately receive a comprehensive diagnostic work-up, including blood work, thoracic radiographs, and, if and when possible, a comprehensive echocardiogram performed by a cardiologist. Alternatively, identification of a normal LA/Ao ratio of 1.2:1 on FCU in a dyspneic feline patient with a history of intermittent coughing episodes may increase the suspicion of primary lower airway disease.
Clinical Indication 2: The Asymptomatic Cat with a Heart Murmur
Another common indication of FCU is the feline patient with an incidental heart murmur in need of general anesthesia. While elective procedures (such as a routine dental procedure) can often be safely delayed for the patient to be first evaluated by a cardiologist, there are many instances in which the clinician has to proceed without a comprehensive cardiac evaluation, such as with emergency procedures. FCU can be advantageous in this setting in that it can quickly help determine the patient’s risk of volume overload and, for the practitioner more experienced in FCU, it may even allow for assessment of the left ventricular wall thickness and systolic function, which provide additional information and may prompt the practitioner to avoid certain anesthetic drugs. In a recent study by Loughran et al., evaluation of the left ventricular wall thickness using FCU by a trained general practitioner was significantly correlated with echocardiographic measurements in cats.
incidental heart murmur in need of general anesthesia. While elective procedures (such as a routine dental procedure) can often be safely delayed for the patient to be first evaluated by a cardiologist, there are many instances in which the clinician has to proceed without a comprehensive cardiac evaluation, such as with emergency procedures. FCU can be advantageous in this setting in that it can quickly help determine the patient’s risk of volume overload and, for the practitioner more experienced in FCU, it may even allow for assessment of the left ventricular wall thickness and systolic function, which provide additional information and may prompt the practitioner to avoid certain anesthetic drugs. In a recent study by Loughran et al., evaluation of the left ventricular wall thickness using FCU by a trained general practitioner was significantly correlated with echocardiographic measurements in cats.
Clinical Indication 3: The Dyspneic Dog
 Left-sided congestive heart failure (LCHF) is common in dogs with heart disease, such as myxomatous mitral valve disease (MMVD) or dilated cardiomyopathy (DCM). FCU can be helpful to increase or lower one’s suspicion of left-sided congestive heart failure, which in dogs manifests as pulmonary edema. Key FCU features include an increased LA/Ao ratio (Figure 1), in combination with numerous B-line artifacts on Vet BLUE lung ultrasound, which, in dogs with LCHF, typically manifests as bilateral, diffuse distribution of infinite coalescing B-lines. Ultimately, thoracic radiographs should be performed to confirm the suspicion of LCHF and monitor the patient’s response to treatment. The reader is also encouraged to pay particular attention to the patient’s signalment and physical exam findings. Typically, advanced MMVD is most common in older, small-breed dogs and is accompanied by a loud left apical systolic murmur. Conversely, DCM is more common in larger-breed dogs, and in these patients, the heart murmur may only be soft or even be absent. Key FCU findings in DCM include left ventricular dilation and severe left ventricular systolic dysfunction.
Left-sided congestive heart failure (LCHF) is common in dogs with heart disease, such as myxomatous mitral valve disease (MMVD) or dilated cardiomyopathy (DCM). FCU can be helpful to increase or lower one’s suspicion of left-sided congestive heart failure, which in dogs manifests as pulmonary edema. Key FCU features include an increased LA/Ao ratio (Figure 1), in combination with numerous B-line artifacts on Vet BLUE lung ultrasound, which, in dogs with LCHF, typically manifests as bilateral, diffuse distribution of infinite coalescing B-lines. Ultimately, thoracic radiographs should be performed to confirm the suspicion of LCHF and monitor the patient’s response to treatment. The reader is also encouraged to pay particular attention to the patient’s signalment and physical exam findings. Typically, advanced MMVD is most common in older, small-breed dogs and is accompanied by a loud left apical systolic murmur. Conversely, DCM is more common in larger-breed dogs, and in these patients, the heart murmur may only be soft or even be absent. Key FCU findings in DCM include left ventricular dilation and severe left ventricular systolic dysfunction.
Dogs with active LCHF are often tachycardic on presentation. However, patients with concurrent sinus node dysfunction or diseases associated with high vagal tone (such as primary respiratory, GI, neurologic, or urinary disease) may not always present with tachycardia.
Another important disease that deserves mention in this section is pulmonary hypertension (PH). While a comprehensive discussion on PH is beyond the scope of this article, dogs with pulmonary hypertension may present with dyspnea, exercise intolerance, and/or syncope, similar to dogs with LCHF. In these cases, however, FCU may identify subjective right heart enlargement and, in some cases of pre-capillary PH without significant concurrent left heart disease, normal LA/Ao ratios.
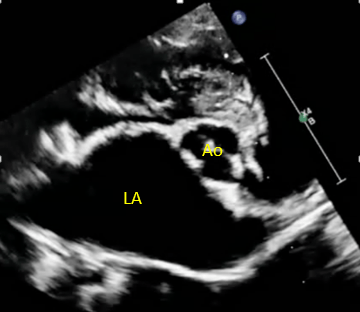
Figure 1: An enlarged left atrium in a dog with advanced MMVD and LCHF. In this case, the LA/Ao ratio was severely increased at 2.3 : 1. LA, left atrium; Ao, aorta.
Limitations of FCU
As mentioned, there are currently no published guidelines on the amount of training required for a practitioner to perform FCU with high proficiency. Additionally, it is vital that the imaging views be obtained in proper imaging planes and the measurements be performed accurately; therefore, FCU performed by an inexperienced clinician may result in inaccurate diagnoses. However, there is growing literature in both human and veterinary medicine showing that, with reasonable training, emergency clinicians and general practitioners can utilize FCU with clinically relevant accuracy in certain settings.
While highly useful in aiding clinical decision-making, FCU should not replace the value of thoracic radiography and a comprehensive echocardiogram.
References
- DeFrancesco TC,Ward JL. Focused canine cardiac ultrasound. Vet Clin North Am Small Anim Pract. 2021; 51: 1203-1216.
- Loughran KL.Focused canine ultrasonography in cats. Vet Clin North Am Small Anim Pract. 2021; 51: 1183-1202.
- Lisciandro, G.R.; Lisciandro, S.C. Lung ultrasound fundamentals, “wet versus dry” lung, signs of consolidation in dogs and cats. Clin. N. Am. Small Anim. Pract. 2021, 51, 1125–1140.
- Lisciandro GR. TFAST Accurate Diagnosis of Pleural and Pericardial Effusion, Caudal Vena Cava in Dogs and Cats. Vet Clin North Am Small Anim Pract 2021; 51: 1169-1182.
- Via G, Hussain A, Wells M, et al. International evidence-based recommendations for focused cardiac ultrasound. J Am Soc Echocardiogr 2014;27(7):683 e1–83 e33.
- Spencer KT, Kimura BJ, Korcarz CE, et al. Focused cardiac ultrasound: recommendations from the American Society of Echocardiography. J Am Soc Echocar- diogr 2013;26(6):567–81.
- Loughran KA, Rush JE, Rozanski EA, et al. The use of focused cardiac ultrasound to screen for occult heart disease in asymptomatic cats. J Vet Intern Med 2019; 33(5):1892–901.
- Boysen SR, Lisciandro GR. The use of ultrasound for dogs and cats in the emergency room: AFAST and TFAST. Vet Clin North Am Small Anim Pract 2013; 43: 773-797.
- Dickson D, Harris J, Chang CH, et al. Validation of a focused echocardiographic training program in first opinion practice. J Vet Intern Med 2022; 36: 1913-1920.
- Tse YC, Rush JE, Cunningham SM, et al. Evaluation of a training course in focused echocardiography for noncardiology house officers. Journal of veterinary emergency and critical care 2013; 23: 268-273.
- Ward JL, Lisciandro GR, Keene BW, et al. Accuracy of point-of-care lung ultrasonography for the diagnosis of cardiogenic pulmonary edema in dogs and cats with acute dyspnea. J Am Vet Med Assoc 2017;250:666–75.
- Ward JL, Lisciandro GR, DeFrancesco TC. Distribution of alveolar-interstitial syndrome in dogs and cats with respiratory distress as assessed by lung ultrasound versus thoracic radiographs. J Vet Emerg Crit Care 2018;28:415–28.
- Ward JL, Lisciandro GR, Ware WA, et al. Evaluation of point-of-care thoracic ultrasound and NT-proBNP for the diagnosis of congestive heart failure in cats with respiratory distress. J Vet Intern Med 2018;32(5):1530–40.
- Janson CO, Hezzell MJ, Oyama MA, et al. Focused cardiac ultrasound and point-of-care NT-proBNP assay in the emergency room for differentiation of cardiac and non-cardiac causes of respiratory distress in cats. J Vet Emerg Crit Care 2020; 30(4):376–83.
- Hezzell MJ, Ostroski C, Oyama MA, et al. Investigation of focused cardiac ultrasound in the emergency room for differentiation of respiratory and cardiac causes of respiratory distress in dogs. J Vet Emerg Crit Care 2020;30(2):159–64.