-
Adopt
-
Veterinary Care
Services
Client Information
- What to Expect – Angell Boston
- Client Rights and Responsibilities
- Payments / Financial Assistance
- Pharmacy
- Client Policies
- Our Doctors
- Grief Support / Counseling
- Directions and Parking
- Helpful “How-to” Pet Care
Online Payments
Emergency: Boston
Emergency: Waltham
Poison Control Hotline
-
Programs & Resources
- Careers
-
Donate Now
 By Nicholas Trout, MA, VET MB, DACVS, ECVS
By Nicholas Trout, MA, VET MB, DACVS, ECVS
angell.org/surgery
surgery@angell.org
617-541-5048
The value and benefits of a thorough and detailed preoperative plan cannot be understated when it comes to canine orthopedic surgery. Thirty years ago, after perusing a couple of radiographs through a well-illuminated viewing box, and maybe making a few notations or measurements with a wax marker, the surgeon would head into the operating room knowing that an appreciation of normal anatomy and an ability to correctly ‘eyeball’ the bone or joint would typically achieve a favorable result. Today, advanced options for corrective surgery in the treatment of joint disease, fractures, and angular limb deformities demand a higher degree of preparation. Thankfully, in the world of digital radiology, software programs have been developed that allow the surgeon to plan, down the millimeter and degree, exactly where to cut, which implant to use, and to see how the postoperative radiographic results will look, with nothing more than a click of a mouse.
At Angell we use vPOP, an orthopedic planning program that is easy to use, offers the ability to cut and reposition bones, and draws from an extensive list of high-definition implants so the surgeon can virtually visualize best type, fit, and position. As long as the radiographs are of good quality and come with appropriately positioned markers to ensure accurate calibration and scale, vPOP can do the rest.
Figure 1 shows a ventro-dorsal pelvic radiograph of a 3.5-year-old castrated male (CM) Catahoula leopard dog that presented with right hind leg lameness secondary to hip dysplasia and secondary osteoarthritis. This radiograph was imported into vPOP, and appropriate femoral stem and acetabular cup implant images moved into place to see which size fit best. Figure 2 shows the immediate postoperative radiograph. vPOP allowed the surgeon to anticipate which instrumentation would be required, improved accuracy of the appropriate osteotomy and, in doing so, likely reduced surgical time.
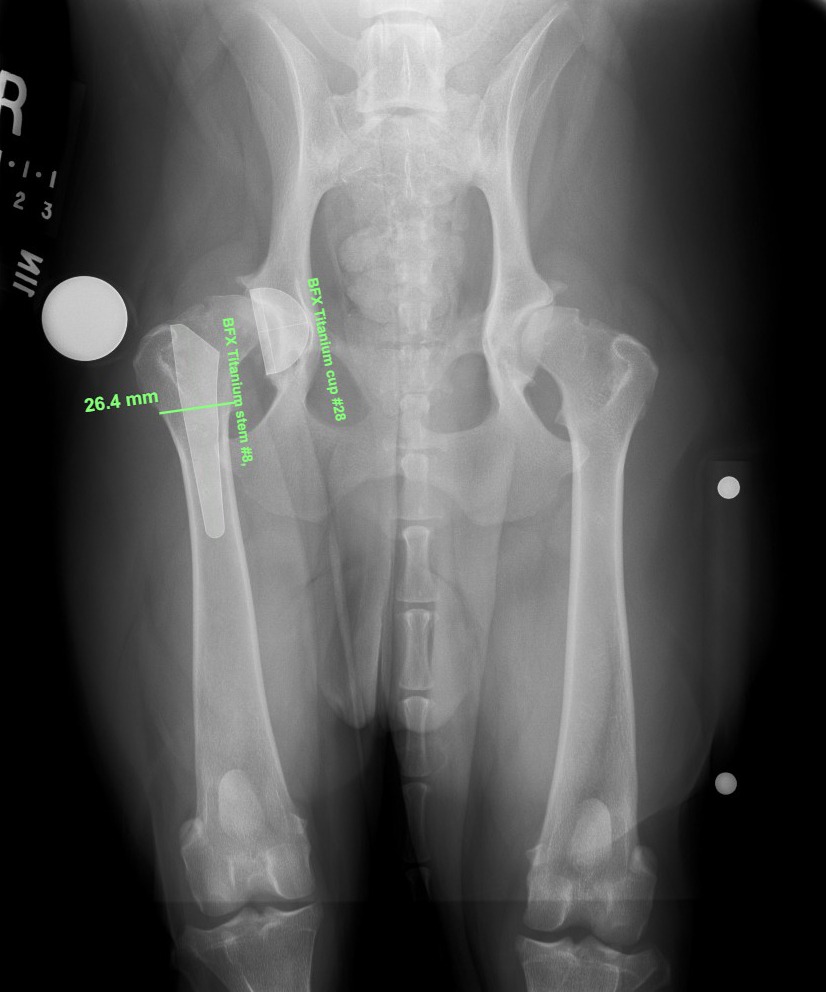 Figure 1: V/D plain radiograph of a total hip replacement candidate showing virtual implant sizes prior to the procedure. |
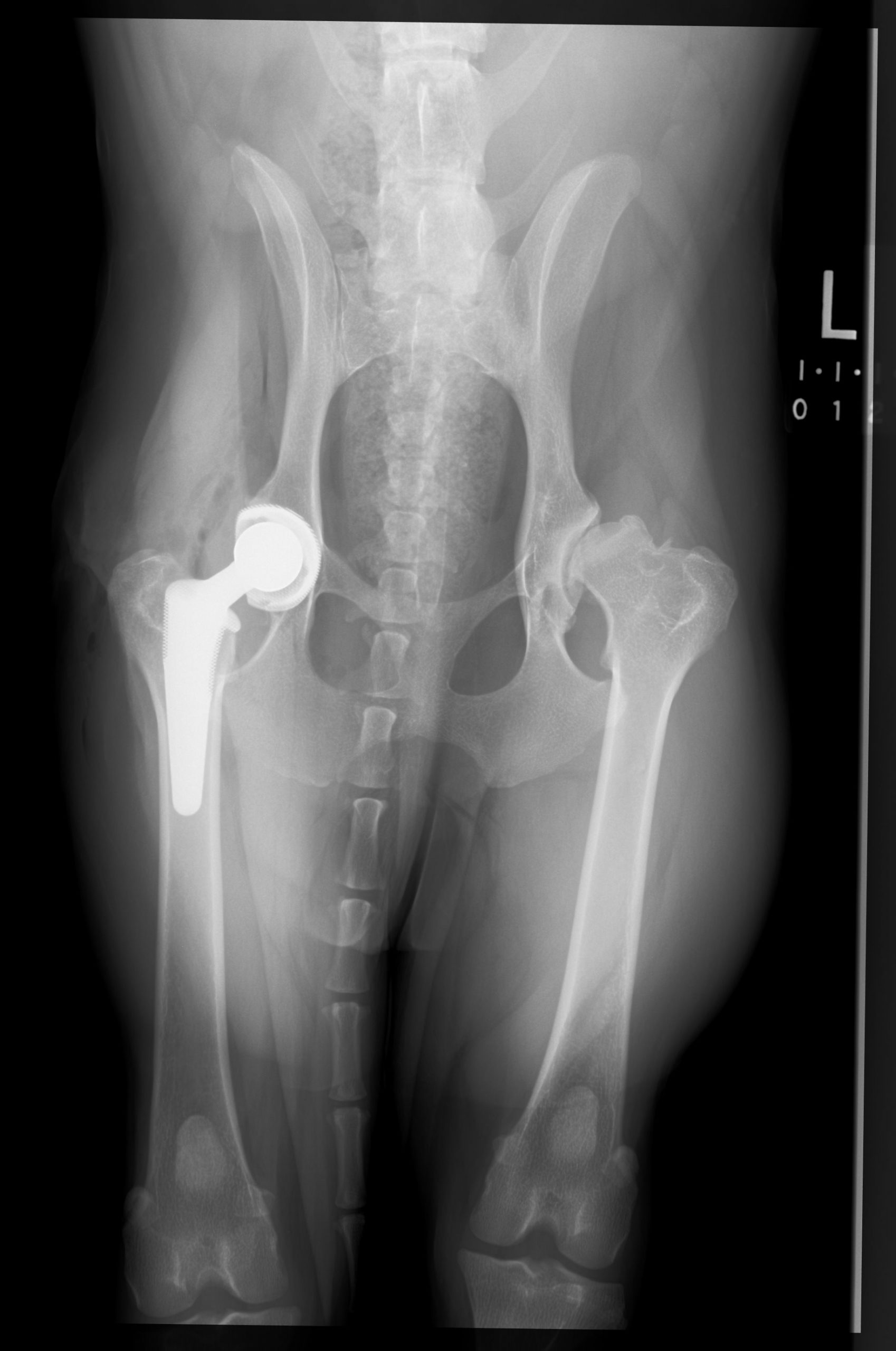 Figure 2: V/D plain radiograph of the postoperative results. |

Figure 3: Lateral radiograph of the proximal tibia, annotated for TPLO.
Figure 3 shows a preoperative plan for a tibial-plateau-leveling osteotomy (TPLO) surgery in a 7-year-old, 12.5kg Cockapoo. Many small active dogs may be better served with a TPLO procedure as an alternative to a lateral suture repair technique however the smaller bone size and implant size makes the margin for surgical error that much smaller. vPOP enabled:
- accurate measurement of the tibial plateau angle (TPA)
- virtual cutting and rotating of the proximal tibia with different sized blades, displaying the amount of rotation required and demonstrating how the cut bone would appear
- allowed for trying different plate sizes to assess best fit
- ensured adequate bone would remain at the tibial crest to minimize the risk of an iatrogenic fracture
All of this information is available in minutes and provides a useful reference to the surgeon during the procedure. By virtue of the AP view (not shown) the surgeon could measure the length of the top screw, minimizing the risk of being too short, and potentially insecure, or too long, and potentially in the joint.

Figure 4: Lateral radiograph of a fractured tibia, offering comparison of implant sizes for internal fixation.
Figure 4 shows a lateral radiograph of a short oblique mid-body tibial fracture and demonstrates the options of a 12 hole or 14 hole plate when considering internal fixation. Again, having this information and decision making allows for shorter surgical time and reduced margins for error.
These examples demonstrate how orthopedic software programs can make planning easier and more accurate, but they can prove invaluable when corrective osteotomies are required. Figures 5 and 6 show the preoperative plan for a CBLO (Cora Based Levelling Osteotomy) with medial closing wedge osteotomy for a three year old Deerhound in which there has been excessive loading on the lateral compartment of the stifle joint exacerbated by a lateral femoral condylar OCD lesion. The dog had also sustained a partially torn cranial cruciate ligament. These images may be busy with colored lines and angles but they provide the surgeon with an essential template, guiding the precise location for an appropriate CBLO cut, the precise angle of the wedge of bone to be removed, and the length of the resulting piece of bone to be excised. Figures 7 and 8 show the postoperative result.
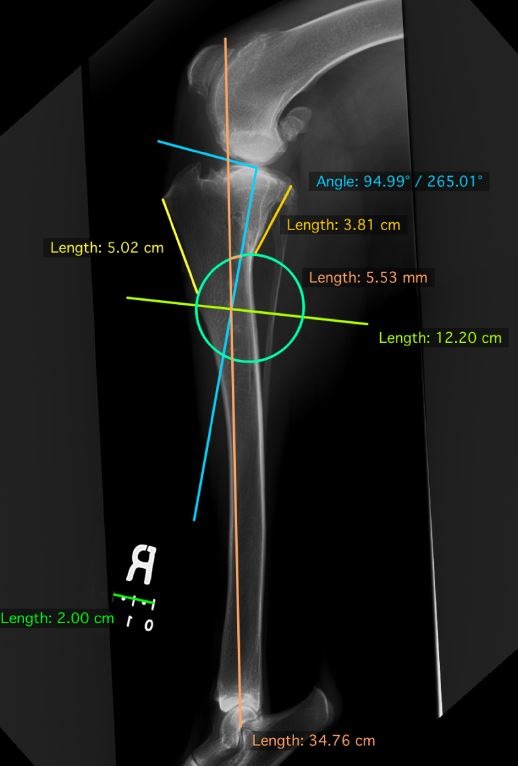 Figure 5: Lateral radiograph of the tibia with planning for CBLO and medial closing wedge osteotomy (credit R.G. Cashmore) |
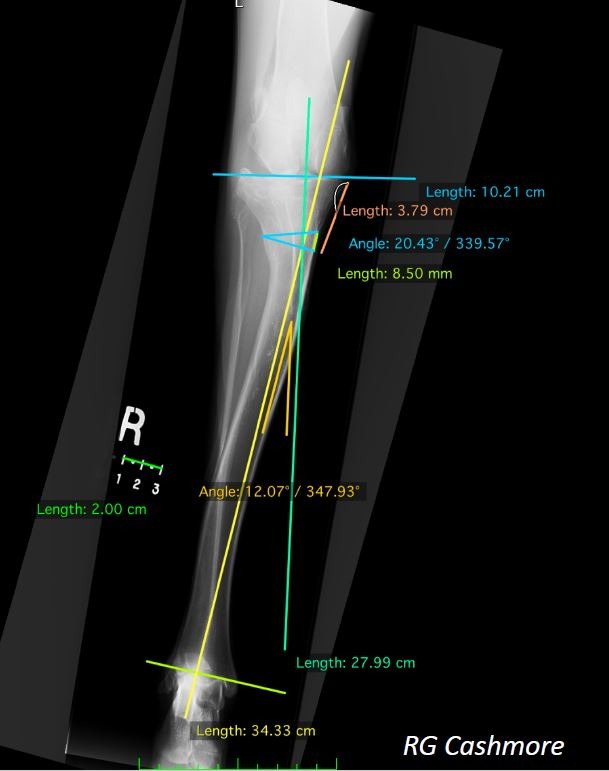 Figure 6: A/P radiograph of the tibia with planning for CBLO and medial closing wedge osteotomy (credit R.G. Cashmore) |
There are many other software programs available, such as Osirix or Horos, and some of these are free or require a nominal annual fee. However, their collective feature is an ability to help the veterinary surgeon plan for any orthopedic procedure, be it simple or complex, aiming to make the ‘real’ surgery, quicker, more accurate, and, hopefully, more reassuring.
 Figure 7: Lateral radiograph of the postoperative osteotomies and fixation. |
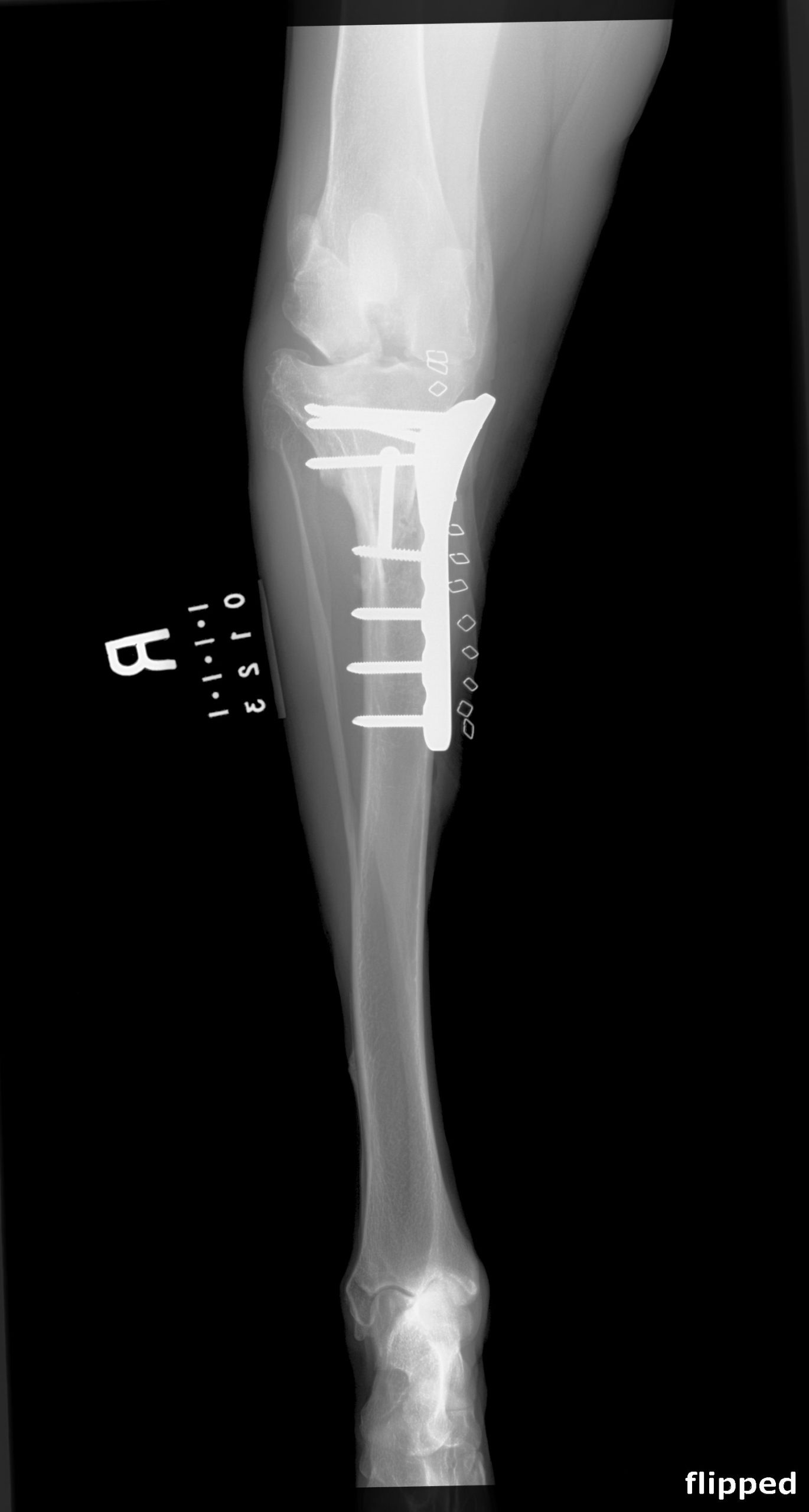 Figure 8: A/P radiograph of the postoperative osteotomies and fixation. |