-
Adopt
-
Veterinary Care
Services
Client Information
- What to Expect – Angell Boston
- Client Rights and Responsibilities
- Payments / Financial Assistance
- Pharmacy
- Client Policies
- Our Doctors
- Grief Support / Counseling
- Directions and Parking
- Helpful “How-to” Pet Care
Online Payments
Emergency: Boston
Emergency: Waltham
Poison Control Hotline
-
Programs & Resources
- Careers
-
Donate Now
 Steven Tsai, DVM, DACVR
Steven Tsai, DVM, DACVR
angell.org/diagnosticimaging
diagnosticimaging@angell.org
617-541-5139
Evaluating a limping dog or cat can be a frustrating and unfruitful exercise, for the veterinarian and client alike. Radiographs of the affected limb will almost certainly be part of the diagnostic workup at some point, and interpreting the radiographs may be similarly frustrating for the primary care veterinarian, radiologist, or surgeon. As with most medical problems, starting with a good history and thorough physical exam (in this case, an orthopedic exam) is an essential baseline. Determining whether the lameness is acute or chronic, intermittent or constant, shifting leg or not, progressive or static will help narrow the list of differentials.

Image 1 – Collimating your x-ray exposure tightly to the area of interest will greatly improve the quality of your radiograph. On the right, attempting to capture both limbs and using very wide collimation results in a poor quality radiograph. On the left, same cat in same position, but with collimation tight over the right carpus.
The most important part of the orthopedic exam (and probably the most important part of the workup) is attempting to localize the cause of lameness to a single joint or single bone. From a radiographic perspective, the reason for this is that the diagnostic quality/yield of your images will be much greater if you are tightly collimated to the area of interest (Image 1). Reducing field of view will reduce x-ray scatter, thereby reducing noise and blurriness. Additionally, focusing on one joint will make it easier to position the patient for straight craniocaudal and lateral views. Significant lesions are frequently missed due to slightly oblique positioning (Image 2).
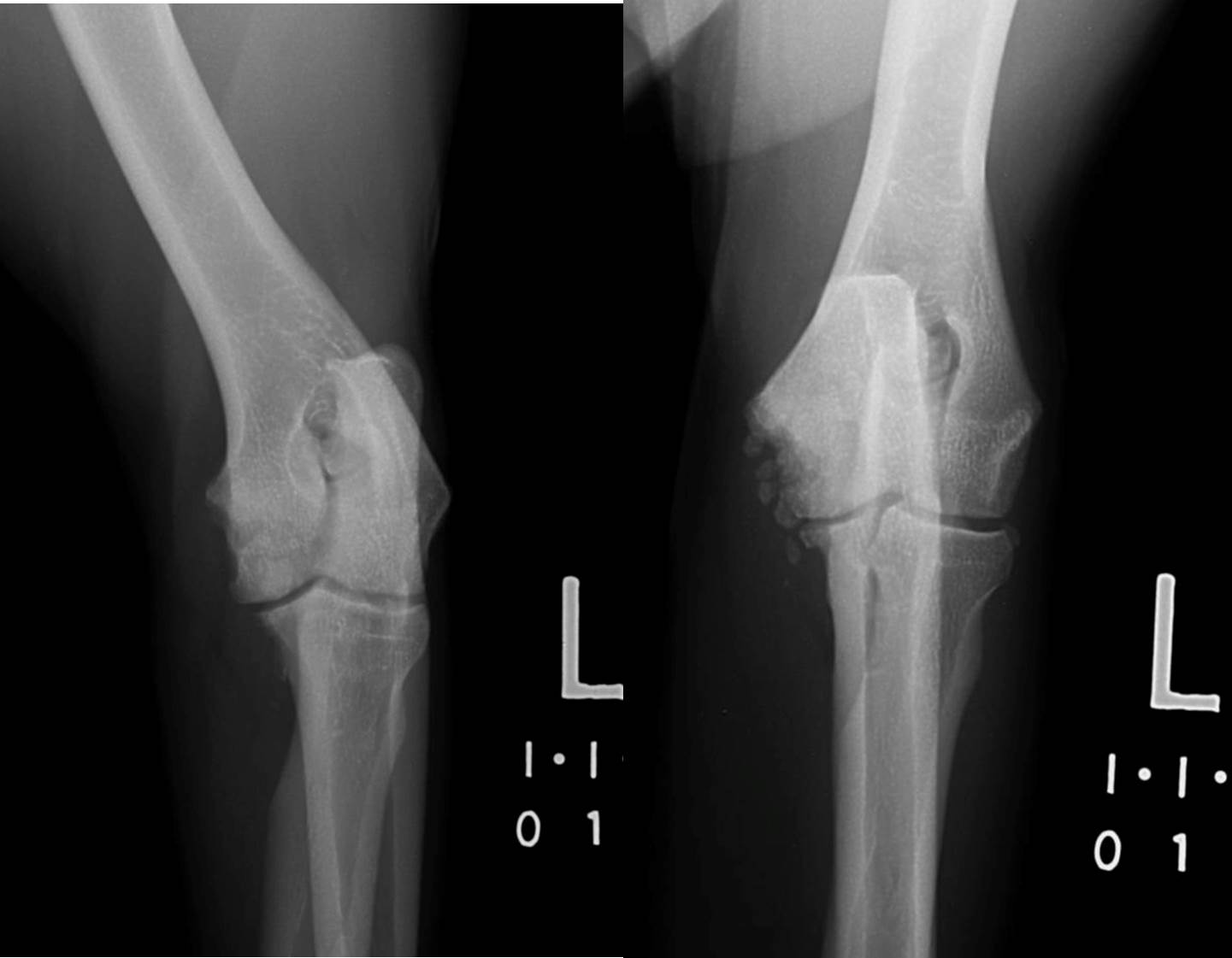
Image 2 – Slight differences in obliquity result in dramatic differences in visibility of lesions. On the left, somewhat obliqued craniocaudal view of an elbow. On the right, straight craniocaudal view of the same elbow, showing fairly severe flexor enthesiopathy and medial coronoid fragmentation.
As with most radiographic interpretation exercises, recognizing what is normal bone and joint anatomy is a prerequisite for determining what is abnormal. A good radiographic atlas is essential for helping to determine whether a bone or joint is normal. The atlas I use most, and probably the textbook I most commonly consult on a regular basis, is “An Atlas of Interpretative Radiographic Anatomy of the Dog and Cat” by Arlene Coulson and Noreen Lewis (Wiley-Blackwell). This atlas includes normal radiographic dog and cat anatomy for adult animals, juveniles at various stages of development, as well as some conformational variants such as chondrodystrophics and brachycephalics. Sometimes if it is unclear whether a particular joint/structure is normal for an individual patient, it can be very useful to obtain a comparison radiograph of the contralateral limb (Image 3).

Image 3 – On the left, carpus of a 4 month old kitten with swelling and lameness. Medial carpal bones appear slightly irregular, but it is not clear whether this is normal incomplete ossification in this young patient (white arrow). Radiograph of the opposite limb confirms that the affected limb is abnormal (osteomyelitis).
Once you have your well positioned, well collimated radiographs centered on the painful joint or bone, the most important question (besides whether an abnormality is present or not), is whether you have an aggressive or non-aggressive lesion. Although many tend to equate an aggressive bone lesion with cancer, technically an aggressive lesion is defined as any process which if left unchecked would progress to complete destruction of bone. In addition to cancer, infection (bacterial or fungal osteomyelitis) and auto-immune disorders (rheumatoid arthritis) can lead to aggressive bone lesions. There are many classic radiographic criteria used to determine presence and severity of an aggressive bone lesion, but typically the two we focus on are presence/pattern of osteolysis and the presence of an ill-defined periosteal reaction.
There are three classic patterns of osteolysis: geographic, moth-eaten, and permeative. Generally speaking the presence of lysis is almost always associated with an aggressive lesion, and the differentiation between the patterns is somewhat academic. The exception is that some benign lesions such as bone cysts may cause focal geographic lysis, which is defined as an area of very well-delineated bone loss, frequently circular or ovoid in contour. Other than these rare exceptions, it is mostly just critical to identify the presence of bone loss, regardless of pattern.
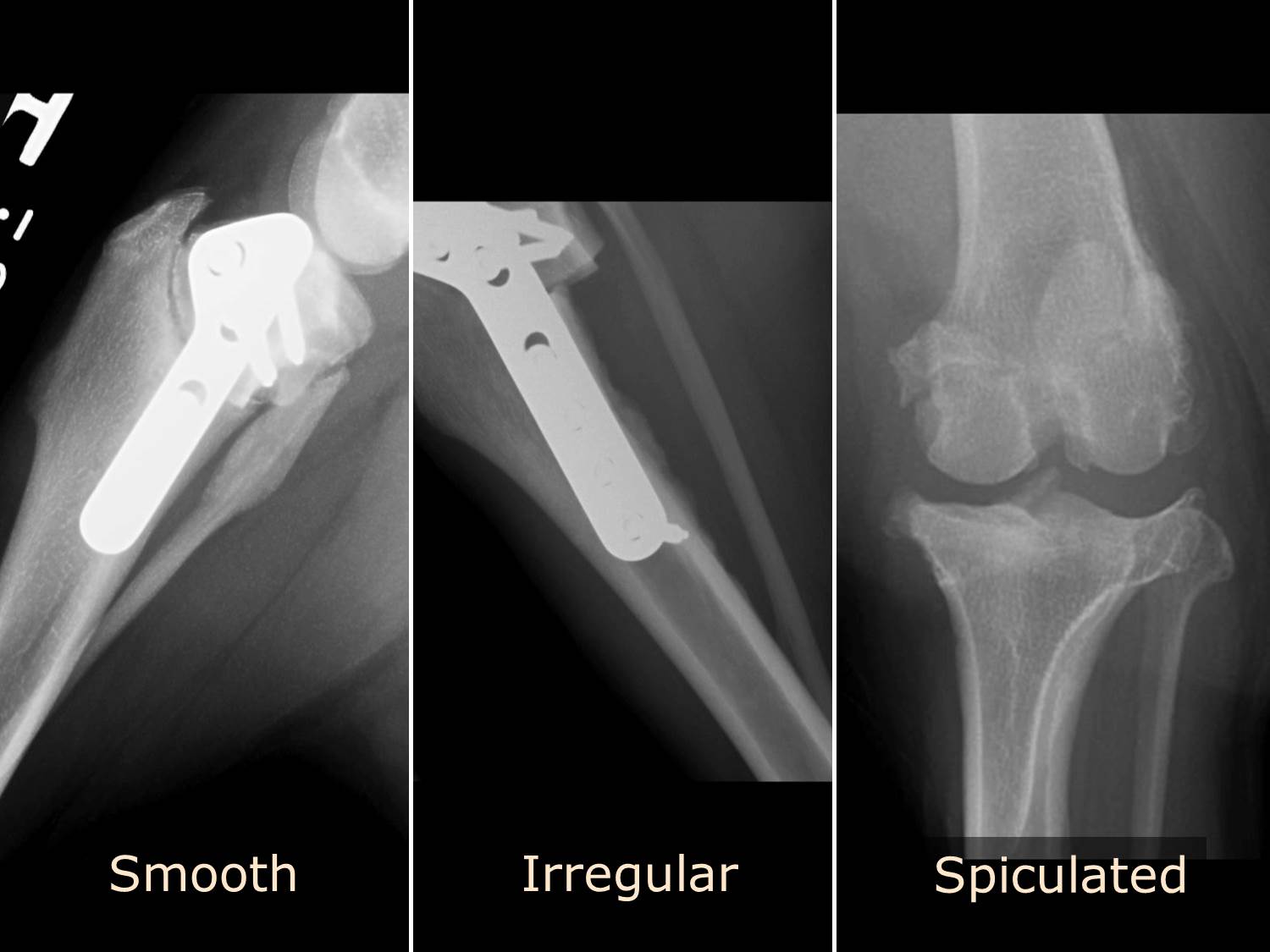
Image 4 – Well defined or uninterrupted periosteal reactions. A smooth periosteal reaction on the proximal fibula secondary to surgical stimulation. An irregular periosteal reaction along the caudal margin of the tibia in a healing TPLO. Spiculated periarticular new bone formation in a stifle with chronic degenerative joint disease.
Periosteal reactions are a bit trickier. Generally speaking, a periosteal reaction is defined as an area of new bone formation occurring along the surface of bone. This is a response of the periosteum surrounding the bone, which tends to lay down new bone as a result of any form of stimulus or injury. With non-aggressive lesions, typically the growth of the lesion is quite slow, and the periosteum is able to lay down new bone in a fairly consistent and organized fashion, leading to a well-defined or uninterrupted pattern (Image 4). With aggressive lesions, the growth rate exceeds the periosteal capacity to produce new bone, and the result is an ill-defined or interrupted pattern (Image 5). One way to help determine whether a periosteal reaction is interrupted or uninterrupted is to imagine using a pencil to trace the contour of the periosteal reaction. If it is possible to trace the entire border of the periosteal reaction without lifting the pencil tip off the radiograph, that is an uninterrupted periosteal reaction.

Image 5 – Ill defined or interrupted periosteal reactions. Lamellar reaction along the medial aspect of the proximal femur, characterized by linear mineralization parallel to the periosteum. Palisading (or columnar) reaction along the distal femur, characterized by linear mineralization perpendicular to the periosteum. Amorphous periosteal reaction associated with a highly aggressive proximal humerus lesion. All lesions were osteosarcoma.
Once you have determined whether an aggressive or nonaggressive bone lesion is present, the differential diagnoses and subsequent case workup should become fairly clear. With an aggressive bone lesion, bone biopsy is typically the next step to assess for malignancy. If there is potential exposure to fungal disease, or if there is the potential for bacterial infection (trauma, previous surgery in the affected area), obtaining bacterial cultures and fungal titers would also be prudent. With nonaggressive lesions, the differentials are most likely going to be related to developmental diseases in young animals and degenerative joint disease in older animals. A thorough discussion of these various orthopedic issues is beyond the scope of this article.
For more information on Angell’s Diagnostic Imaging service or our online imaging consultative services, please visit angell.org/diagnosticimaging. Dr. Tsai can be reached at 617-541-5139 or via e-mail (diagnosticimaging@angell.org).