-
Adopt
-
Veterinary Care
Services
Client Information
- What to Expect – Angell Boston
- Client Rights and Responsibilities
- Payments / Financial Assistance
- Pharmacy
- Client Policies
- Our Doctors
- Grief Support / Counseling
- Directions and Parking
- Helpful “How-to” Pet Care
Online Payments
Emergency: Boston
Emergency: Waltham
Poison Control Hotline
-
Programs & Resources
- Careers
-
Donate Now
 Dan Biros, DVM, DACVO
Dan Biros, DVM, DACVO
angell.org/eyes
ophthalmology@angell.org
617-541-5095
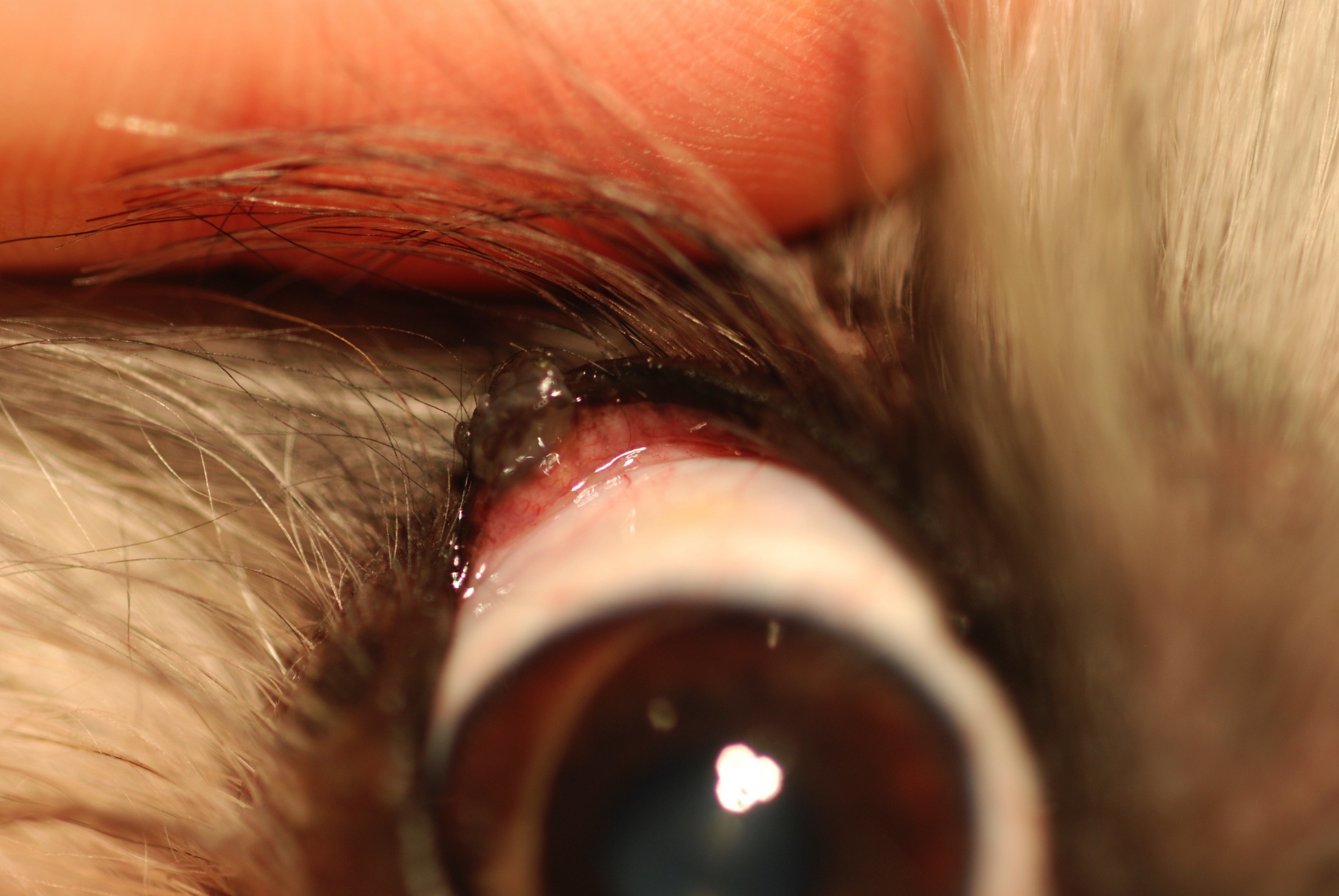
Figure 1. Eyelid Meibomian adenoma amenable to V-plasty correction.
The most common type of elective surgery we perform at Angell Ophthalmology is removal of small eyelid tumors via V-plasty. Eyelid tumors can occur in any breed at any age but older dogs tend to present to our service for evaluation. The most common types of tumors appear as neoplasia of the Meibomian gland, the primary oil producing glands located in the eyelid margin. There are dozens of these glands in each eyelid, and the origin of these tumors is usually either the duct linings (epithelioma) or the ascini (adenoma) that grow as multilobulated pink to grey well vascularized (Figure 1). Less common benign tumors that have been reported with any significant frequency include papillomas and melanocytomas. Fortunately, for most dogs, the vast majority of eyelid margin tumors are benign so there is little risk for metastases, and surgery is usually curative. The lesions if left alone, however, have the potential to be locally aggressive and disfiguring leading to ocular surface irritation or worse, corneal ulceration or infection. Depending on the size of the tumor there are options for surgical resection, especially if the mass is progressing in size or associated with ocular surface disease.

Figure 2. Cryosurgery for small eyelid margin tumor.
Determining when the eyelid surgery is indicated depends on location, size, and rate of growth. If the rate of growth is slow and there is minimal if any redness or discharge, periodic observation may be sufficient for monitoring change including progressive ocular surface irritation especially if the patient is deemed high anesthetic risk. If the eyelid tumor is smaller than 2-3 mm then observation is indicated, however we often will advocate for early tumor removal if possible to reduce morbidity and preserve as much of the normal eyelid margin as possible. For small tumors, cryosurgery can be very effective. It is a suture-less procedure that requires a brief general anesthesia. Typically the tumor is trimmed to the eyelid margin surface (submitted to pathology in most cases), and the affected eyelid is treated with two rounds of freezing with a cryoprobe, about 20 seconds each treatment. Protecting the skin and globe is essential anytime there is eyelid cryosurgery. Towels and a corneal shield are us ed for this purpose. A chalazion clamp is very helpful to immobilize the eyelid during cryosurgery and will help expose the conjunctival surface of the eyelid margin where the cryoprobe is applied just below the eyelid margin for 20 seconds (from visible ice formation in the eyelid) (Figure 2). Depigmentaion (sometimes permanent), transient blepharitis, blepharedema, and skin ulceration is expected with cryosurgery and can last up to 7-10 days peaking about 3-5 days post surgery on average. Some local skin ulceration may also occur and resolves in the first 1-2 weeks. The goal of care is to destroy any residual tumor cells and allow the eyelid to heal without any incisions or suture placement. Infection is rare but topical antibiotics and systemic anti-inflammatories and pain medication is typically used postoperatively. CO2 laser has also been used for small eyelid tumors.
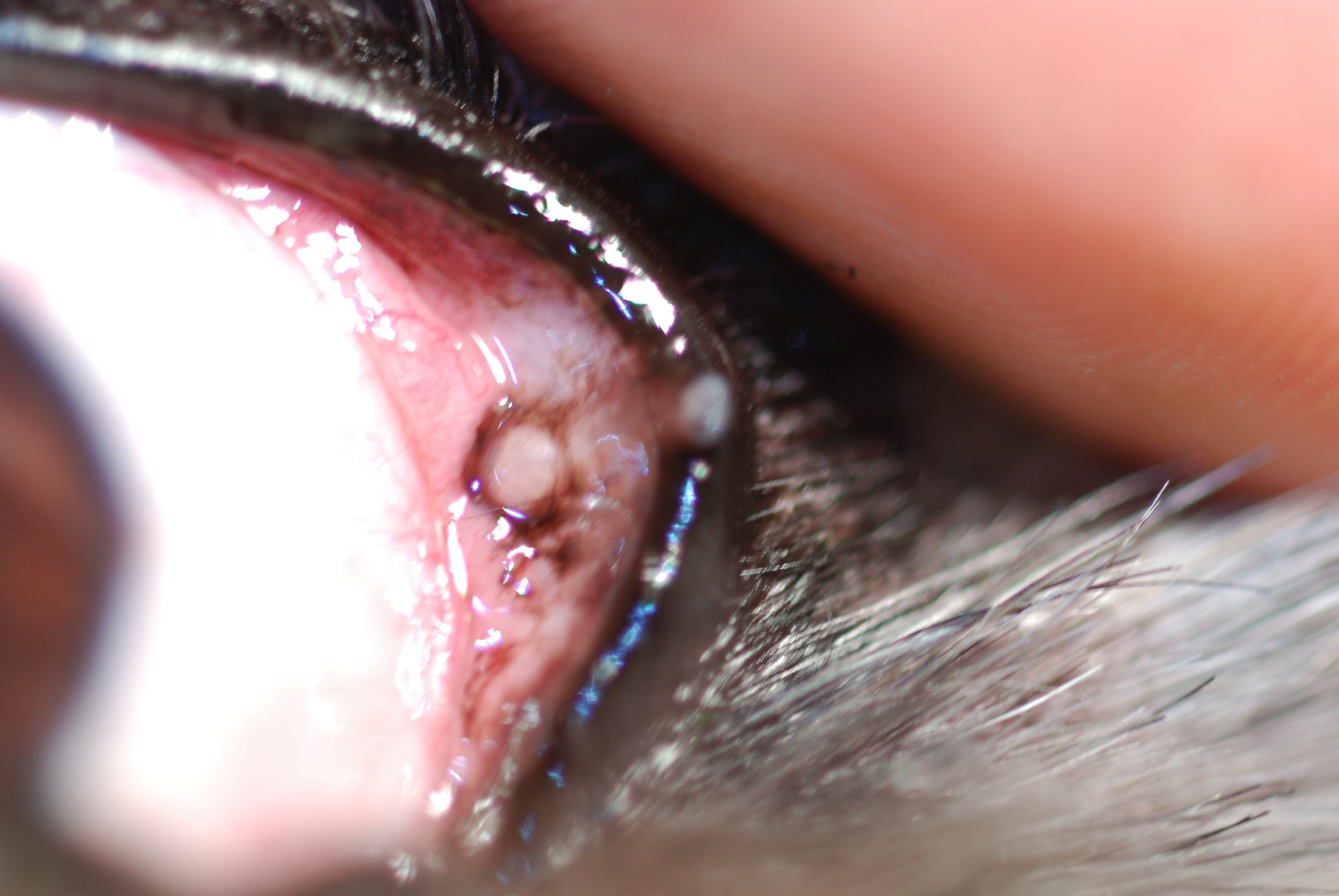
Figure 3. Small eyelid margin tumor with deeper chalazion (to the left of the margin tumor) seen on conjunctival surface.
While cryosurgery is generally done by a veterinary ophthalmologist, surgical resection for margin tumors is not uncommonly done by ophthalmologists and general practitioners alike. For tumors up to 8-9 mm in diameter, eyelid V-plasty under brief general anesthesia can be a successful way to resolve larger eyelid tumors with or without chalazion formation. Chalazion are ruptured Meibomian glands that cause local inflammation in the region of the primary tumor (Figure 3).
Lipogranulomatous blepharitis (a.k.a. chalazion) is frequently an accompanying diagnosis for many of our eyelid margin tumor biopsies. Simple V-plasty requires sharp resection of the mass with a size 15 surgical blade while the eyelid is immobilized with a chalazion clamp, usually the open side to the conjunctival surface, but this can vary depending on the orientation of the tumor. Closure is accomplished with a soft braided suture such as 4-0 silk (non absorbable) or 4-0 vicryl (absorbable) depending on the surgeon’s preference. To reconstruct a fluid eyelid margin and preserve good eyelid conformation, a figure of 8 pattern is recommend followed by simple interrupted or cruciate patterns to close the remaining surgical incision (Figure 4).
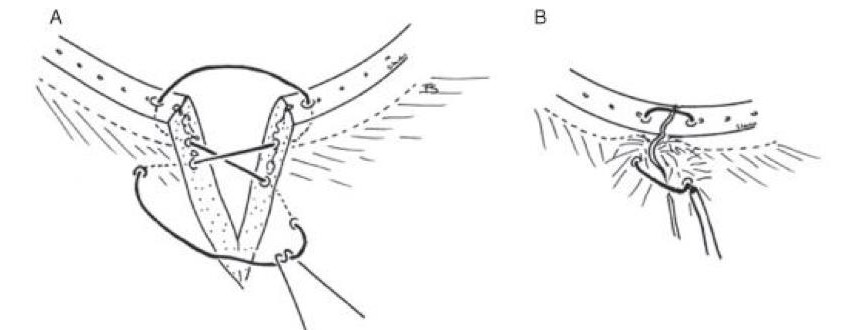
Figure 4. Figure of 8 suture pattern for closure of the V-plasty
Usually for dogs and cats a single layer closure is sufficient. If more suture support is needed a deeper layer of 5-0 or 6-0 vicryl can be placed prior to the skin sutures to bring the surgical incision together and provide added strength. Simple continuous or simple interrupted patterns are commonly used, but care must be taken to avoid suture exposure on the conjunctival surface. Complications from V-plasty can be minor or severe and may include corneal ulceration, infection, suture reaction, eyelid margin misalignment, or eyelid tumor regrowth if tumor cells are left behind.
When an eyelid tumor is suspected to be malignant: Types of more malignant tumors on the eyelid include squamous cell carcinoma, melanoma, sarcoma and mast cell tumors. These tumors need a more careful work up often including a confirmatory biopsy or aspirate prior to definitive resection, since surgical margin size and careful eyelid margin reconstruction are integral parts of the procedure to preserve vision and comfort. Systemic bloodwork, lymph node examination, and chest x-rays are also important prior to any elective surgery for possible metastatic or malignant cancer. There are surgical options for malignant tumors and benign tumors larger than 10 mm that offer more suitable reconstruction than V-plasty can provide. These options include rotating skin grafts, H-plasty, and Z plasty most frequently performed by ophthalmologists or surgeons.
When there is concurrent ocular surface disease or suspected swelling from noncancerous focal blepharitis: Patients with allergies or concurrent dry eye deserve extra attention to perioperative corneal health as eyelid irritation can exacerbate a sensitive ocular surface. In these higher risk patients utmost attention to suture placement and generous use of postoperative medicated lubricants and medication to support tear production should be used without interruption. In general 4-6 times daily for topical antibiotics including neopolybac or erythromycin are used for uncompl

Figure 5, Inflammatory eyelid lesion (mixed inflammation on cytology) in a Boston terrior. The lesion resolved with topical anti-inflammatories.
icated eyelid tumors where the ocular surface is stable. Pain management with a short course of oral NSAID is also indicated as is use of an E-collar for up to 2 weeks. Some eyelid lesions are also inflammatory and do not need surgery for resolution (Figure 5).
Topical neopolydex applied directly on the lesion 2-3 times daily for up to 10-14 days usually provides adequate treatment for these conditions. However, some more persistent lesions require more frequent application of the anti-inflammatory or oral steroids and antibiotics in select cases (e.g. Staph blepharitis). FNA cytology of the lesions can direct the therapy in more stubborn swellings, and can also disclose more sinister conditions including mast cell tumors. Histiocytomas have also been reported near the eyelid margin and often resolve on their own with time and supportive care. Styes are less frequent and are simply a chalazion with a bacterial infection. Treatment can be from lancing and local +/- systemic antibacterials in addition to local anti-inflammatories (e.g. neopolydex).
In summary, many bonafide eyelid masses can be successfully treated with simple surgery. Their appearance is typically spontaneous and unpredictable, but more common in older patients. Considerable care to preserve the eyelid margin continuity will greatly reduce the risk for ocular surface complications in the short and long term, and is essential for eyelid function. All eyelid tumors can be addressed with the help of veterinary ophthalmologists although some smaller tumors can be handled in the care of the primary veterinarian comfortable in eyelid margin surgery.
For more information about Angell’s Ophthalmology service, please visit www.angell.org/eyes. Dr. Biros can be reached for consults or referrals at 617-541-5095 or ophthalmology@angell.org
Resources:
- Essentials of Veterinary Ophthalmology by Kirk N. Gelatt Wiley-Blackwell
- Veterinary Ophthalmic Surgery, 1e by Kirk N. Gelatt VMD, Janice P. Gelatt MFA Elsevier
- Slatter’s Fundamentals of Veterinary Ophthalmology by David Maggs BVSc(Hons) DAVCO, Paul Miller DVM DACVO Elsevier (Saunders)
- Evaluation of one- vs. two-layered closure after wedge excision of 43 eyelid tumors in dogs. Romkes G, Klopfleisch R, Eule JC.
- Vet Ophthalmol. 2014 Jan;17(1):32-40. doi: 10.1111/vop.12033. Epub 2013 Feb 13.