-
Adopt
-
Veterinary Care
Services
Client Information
- What to Expect – Angell Boston
- Client Rights and Responsibilities
- Payments / Financial Assistance
- Pharmacy
- Client Policies
- Our Doctors
- Grief Support / Counseling
- Directions and Parking
- Helpful “How-to” Pet Care
Online Payments
Emergency: Boston
Emergency: Waltham
Poison Control Hotline
-
Programs & Resources
- Careers
-
Donate Now
 By Shawn Kearns, DVM, DACVIM
By Shawn Kearns, DVM, DACVIM
Angell Internal Medicine
617-541-5186
www.angell.org/internalmedicine
Canine hyperadrenocorticism (HAC), or Cushing’s disease, is an endocrine disease affecting primarily older dogs with 80–85% of cases caused by pituitary-dependent disease (PDH); the remainder are due to an adrenocortical tumor (AT). There is a slightly increased predisposition for females (55–65%) and larger breeds may be affected more frequently with an AT.

Figures 1 and 2: The two images here represent dorsal and sagittal views from CT scan of a patient with bilateral adrenomegaly. Ultrasound was concerning but not definitive for vena caval invasion. CT confirmed vena cava invasion.
We are all familiar with the common clinical signs of HAC as well as laboratory findings so those will not be discussed in this article. If a single sign compatible with HAC is present, it is likely to be either polyuria/polydipsia or skin coat changes. Less commonly seen signs include those related to a macrotumor (behavior change, inappetance, obtundation, aggressiveness, apparent blindness and seizures), though sometimes signs are subtle. About 10-25% of dogs will develop neurologic signs months to years after the initial diagnosis. Other less common signs include anestrus, testicular atrophy, ligament laxity, facial palsy, spontaneous thromboembolism and cortisol induced insulin resistance. Signs from an invasive adrenocortical carcinoma may include hemorrhage due to vessel invasion or thrombosis of the vessel (ascites, hind limb edema or paresis). If less common clinical presentations are identified first, a thorough review of the history, physical examination findings, and routine laboratory test results may provide additional evidence for HAC.
A recent Consensus statement was published in the Journal of Veterinary Internal Medicine (JVIM 2013; 27: 1292-1304): so the remainder of this article will focus on the panel recommendations in regards to testing for HAC. Testing should only be considered if there are clinical signs (common or uncommon). Biochemical panel, complete blood cell counts, urinalysis, UPC and blood pressure results by themselves are not indications to test.
No test is 100% diagnostic for HAC. Diagnosis depends on documenting increased cortisol production (ACTH stimulation) or decreased sensitivity of the hypothalamic-pituitary-adrenal axis (HPPA) to the normal negative feedback of steroids administration (Low-dose dexamethasone suppression test; LDDST). Reference ranges may need re-evaluation in the future as we are likely testing sooner and ranges were generated many years ago. If a patient tests negative, repeat testing in 3-6 months may be warranted especially if signs progress.
The LDDST is currently considered the screening test of choice unless iatrogenic HAC is a consideration. The cortisol concentration at 8 hours after dexamethasone administration is used to diagnose HAC. In the clinical experience of the Panel, normal dogs are usually below or close to the detection limit of the sample (i.e. < 1.0). Therefore if a patient is below 1.4 but not below the detection limit, HAC may still be considered. In addition, an inverse pattern where the 4 hour cortisol is high but the 8 hour is below the detection limit may also indicate HAC. Results should be interpreted with caution if the patient is currently taking phenobarbital as those dogs occasionally will not show suppression.
The ACTH stimulation test has a lower sensitivity (range 57-95%) so is considered inferior to the LDDST as a screening test but is the test of choice for iatrogenic HAC. Synthetic ACTH is recommended over compounded drug and intravenous administration is preferred over intramuscular. Progestagens, glucocorticoids, and ketoconazole all suppress the HPAA axis and response to ACTH. Phenobarbital does not appear to affect the test.
The urine corticoid: creatinine ratio (UCCR) is a sensitive test (75%-100%) for detection of cortisol hypersecretion but is influenced by endogenous stress and non-adrenal illness. Collection should take place at home, at least 2 days after a veterinary visit, to decrease the likelihood of false positives.
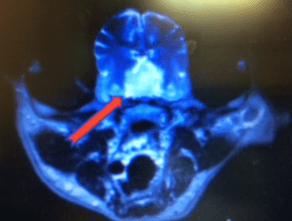
Figure 3: CT image of a pituitary macroadenoma. The patient was displaying behavioral changes and was not eating well each time trilostane was restarted despite a normal ACTH stimulation.
Differentiating tests should only be pursued once there has been a positive on a screening test. The canine ACTH measurement is the most accurate stand-alone biochemical test for differentiation, however, reference ranges vary by technique and certain assays are less sensitive. In addition, proper sample handling is crucial to accurate results. Discordant results can occur and many dogs with PDH will have ACTH at the lower end of the reference range but they should not be lower than the low end reference range. The high dose dexamethasone suppression test (HDDST) can be used to differentiate PDH from AT. If suppression occurs, the patient likely has PDH. However, if there is no suppression, it should be kept in mind that about 25% of PDH dogs will not suppress even at the higher dose. A macroadenoma may be more likely in a dog without an AT that does not suppress on the HDDST.
For those patients who cannot be hospitalized, an oral dexamethasone suppression test can be considered. Samples for UCCR are taken on 2 consecutive days and then 3 doses of dexamethasone (0.1mg/kg PO) are given at 6- 8 hour intervals and urine collected again the following day. A decrease in the UCCR to < 50% of the mean basal values is consistent with PDH. Lack of suppression does not discriminate between PDH or AT. Changes in metabolism of dexamethasone may influence the results of any of the suppression tests.
Imaging must be used in conjunction with hormonal testing and should not be used as the sole modality for diagnosis. Radiographic changes in patients with HAC include abdominal distention, good contrast due to fat deposition, hepatomegaly, bladder distention, mineralization of the bronchi and pulmonary interstitium, and possibly a mass effect or mineralization in the retroperitoneal space. On US, adrenal gland width is considered the most informative parameter but breed and body size related differences must be considered. US can estimate tumor size and possibly vascular or soft tissue invasion, however, CT scan and MRI are more sensitive for evaluation of invasiveness as well as metastases (see Figures 1 and 2). Metastases, venal cava invasion by a tumor mass, adrenal width (> 4cm), or a combination of these findings is highly suggestive of malignancy.
Because radiation therapy or hypophysectomy are the required treatment for macro-tumors and both are more effective with smaller tumors and in the absence of neurologic signs, the Panel recommends pituitary imaging be considered for all dogs at the time of initial diagnosis (see figure 3). Of course, if clinical signs suggest a macro-tumor, CT or MRI is also recommended. As pituitary tumors and a cortisol secreting AT may be present at the same time, some also recommend pituitary imaging with AT.
If a patient does not fit the clinical picture for HAC, testing for occult HAC (“atypical HAC”) should not be considered. While a cause and effect relationship between AT sex hormones and clinical signs is well documented, a causative relationship with sex hormones and PDH has not been established. Therefore, an adrenal sex hormone panel should be considered for patients with inappropriately low cortisol levels on initial screening tests and with adrenal tumors not testing positive for cortisol secretion. Food stimulated HAC should also be a differential when considering occult HAC, especially if the fasting cortisol concentration is low.
In conclusion:
Endocrine testing for HAC should only be considered if there are compatible physical exam findings and history. Testing should not be performed based on laboratory changes alone
The LDDST is considered the screening test of choice
An endogenous ACTH level or abdominal ultrasound are recommended for differentiating between AT and PDH
Sex hormone testing is recommended mainly when an adrenal tumor is present and the initial cortisol testing has returned low
For more information, please contact Angell’s Internal Medicine service at 617-541-5186 or internalmedicine@angell.org.